1. A 34-year-old man complains of pale edema of the face, feet, shins, and lumbar area, elevated blood pressure up to 160/100 mm Hg, and general weakness. He has a clinical history of nonspecific ulcerative colitis. Objectively: pulse - 84/min., rhythmic, blood pressure - 165/100 mm Hg; edemas all over the body; the skin is pale and dry, with low turgor. The kidneys cannot be palpated, on an attempt to palpate them they are painless. Blood test: erythrocytes - 3.0∙1012/L, Hb - 100 g/L, erythrocyte sedimentation rate - 50 mm/hour. Urinalysis: proteins - 3.5 g/L, erythrocytes - 7-10 in the vision field, leukocytes - 5-6 in the vision field. Daily proteinuria - 6 grams. What analysis should be conducted additionally to verify the diagnosis?
2. After overexposure to cold a 45-year- old woman developed acute pain in her suprapubic and
lumbar areas during urination, sharp pains at the end of urination, false urges to urinate. Urine is
turbid with blood streaks. The doctor suspects urinary tract infection. What results of laboratory
analysis would be the most indicative of such infection?
Explanation
Urinary tract infections are commonly associated with dysuria, urinary frequency, urinary urgency and lumboabdominal pains.
When you have a UTI, the lining of the bladder and urethra become inflammed and irritated just as your throat does when you have phrayngitis, common cold - upper respiratory tract infections. The irritation can cause pain in your lower abdomen - pelvic area and even lower back, and will usually make you feel like urinating more often (false urges). Burning or pain when urinating is the most common symptom. You may even feel a strong urge or need to urinate but only get a few drops. This is because the bladder is so irritated that it makes you feel like you have to urinate, even when you don't have much urine in your bladder. UTIs can be found by analyzing a urine sample for Urine Microscopy/Culture/Sensitivity (Urine M/C/S). The urine is examined under a microscope for bacteria or white blood cells (leukocyturia), which are signs of infection. Blood can also be found in the urine sample (hematuria); this can be due to an infective or mechanical cause.
The other options given are more specific for kidney pathologies - proteinuria, gross hematuria, creatinine and urea. Rarely are they elevated in pathologies relating to Urinary Tract Infections except in cases where UTI’s become complicated and the kidney is affected after a prolonged and untreated UTI.
3. A 40-year-old man with Bekhterev disease (ankylosing spondylitis) complains of elevated body
temperature up to 37.8°C, back pain and stiffness, especially observed during the second half of
the night. This condition has been lasting for 2 years. Objectively: reduced spinal mobility, painful
sacroiliac joint, erythrocyte sedimentation rate - 45 mm/hour. X-ray shows narrowing of the
intervertebral disc space and of the sacroiliac joint. What eye pathology is often associated with this
type of disease progression?
4. A 27-year-old man complains of pain in his leg joints, purulent discharge from the eyes, and painful
burning sensations during urination. Disease onset was acute. He has a history of influenza. The
patient smokes and drinks alcohol in excess. In his line of work he is often away on business trips.
What is the most likely etiological factor of this disease?
Explanation
Reactive arthritis is an inflammatory arthritis which manifests after several days to weeks after a gastrointestinal or genitourinary infection. It is also described as a classic triad of arthritis, urethritis and conjunctivitis. However, a majority of patients do not present with the classic triad. It was previously called "Reiter syndrome."
Classic triad:
Conjunctivitis: purulent discharge from the eyes
Urethritis: painful burning sensations during urination
Arthritis: pain in leg joints
Reactive arthritis is known to be triggered by a bacterial infection, particularly of the genitourinary (Chlamydia trachomatis, Neisseria gonorrhoeae, Mycoplasma hominis, and Ureaplasma urealyticum) or gastrointestinal (GI) tract (Salmonella enteritidis, Shigella flexneri, and dysenteriae, Yersinia enterocolitica, Campylobacter jejuni, Clostridium difficile).
The classic triad can be remembered using this:
Conjunctivitis; Urethritis; Arthritis - Can’t See; can’t pee, can’t bend my knee
5. After a long drive with the window open a man developed facial asymmetry; he cannot close his
right eye, his right nasolabial fold is smoothed out, movements of expression are absent on the
right, there is a disturbance of gustatory sensation in the tongue on the right. No other neurological
pathologies were detected. What disease can be provisionally diagnosed in this patient?
6. During an outdoors school event in hot weather, a 10-year-old girl lost her consciousness. Body
temperature - 36.7°C. Objectively her skin is pale and cold to touch, her pupils are dilated. Blood
pressure - 90/50 mm Hg. Heart rate - 58/min. What pathology occurred in this case?
7. A 47-year-old man developed the signs of decompensated laryngeal stenosis against the
background of acute flegmonous laryngitis. He presents with inspiratory dyspnea at rest, forced
position, cyanotic skin covered in cold sweat, tachycardia, deficient pulse, and low blood pressure.
What urgent treatment tactics should be chosen?
8. 10 hours after birth a child developed jaundice, hypotonia, hyporeflexia, and moderate
hepatosplenomegaly. Feces and urine are of normal color. Umbilical cord blood bilirubin is 51
mcmol/L due to unconjugated bilirubin levels. In venous blood: erythrocytes - 3.5∙1012/L, Hb - 140
g/L, reticulocytes - 1.5%, bilirubin - 111 mcmol/L, conjugated - 11 mcmol/L, ALT - 40 U/L, AST - 30
U/L. Mother’s blood group is A(II) Rh(-), child’s blood group is A(II) Rh(+). What laboratory test can
confirm the diagnosis?
9. A 51-year-old man complains of vomiting with blood. He has been drinking alcohol excessively.
Health disorder has been observed since he was 40, when he first developed jaundice. On
examination the skin and visible mucosa are icteric, with a stellate vascular pattern. The patient is
malnourished and presents with abdominal distension, umbilical hernia, and ascites. The edge of
the liver is tapered and painless, +3 cm, the spleen is +2 cm. Blood test: Hb - 80 g/L, leukocytes -
3∙109/L, platelets - 85∙109/L. What is the cause of portal hypertension in this patient?
Explanation
Cirrhosis is a complication of liver disease that involves loss of liver cells and irreversible scarring of the liver. The scarring is accompanied by loss of functioning liver cells. Cirrhosis is usually a late-stage disease of the liver that is not reversible in severe cases.
Hepatitis B, C, and chronic alcohol abuse are frequent causes (Question stem - patient takes alcohol excessively). Initially patients may experience fatigue, weakness and weight loss. During later stages, patients may develop jaundice (yellowing of the skin), gastrointestinal bleeding, abdominal swelling and confusion.
The most common cause of portal hypertension is cirrhosis of the liver. Portal hypertension is an increase in the blood pressure within a system of veins called the portal venous system. Veins coming from the stomach, intestine, spleen, and pancreas merge into the portal vein, which then branches into smaller vessels and travels through the liver. If the vessels in the liver are blocked due to liver damage, blood cannot flow properly through the liver. As a result, high pressure in the portal system develops.
Budd-Chiari syndrome is a condition in which the hepatic veins (veins that drain the liver) are blocked or narrowed by a clot (mass of blood cells). It may lead to portal hypertension, ascites, cirrhosis etc. Budd-Chiari syndrome can be caused by conditions and situations that cause your blood to clot (form a blockage) like sickle cell disease, pregnancy, myeloproliferative disorders. It is not caused by excessive alcohol intake or Hepatitis.
Hemochromatosis, Constrictive Pericarditis and Thrombosis of the splenic vein will not directly lead to portal hypertension.
10. An 18-year-old patient always obeys others and adapts his needs to the demands of the people on
whom he depends. He excessively defers to their wishes and makes them responsible for his
wellbeing, cannot defend his interests and needs support from other people. Such psychic profile
has been formed in the childhood, remains unchanged, and hinders adaptation. What psychic
disorder is observed in this patient?
11. A 45-year-old man with thrombophlebitis of the deep veins in his legs suddenly after physical
exertion developed sharp pain in his thorax on the right, dyspnea, and hemoptysis. Objectively his
condition is severe; he presents with acrocyanosis, shortening of pulmonary percussion sound on
the right, and weakened respiration. Respiration is 30/min., blood pressure is 110/80 mm Hg. ECG
shows sinus tachycardia, heart rate is 120/min., electrical axis of the heart deviates to the right, SI-
QIII. What is the most likely diagnosis?
12. A 15-year-old girl complains of dizziness and sensation of lack of air that she develops in
emotionally straining situations. Relief occurs after she takes corvalol. Objectively: hyperhidrosis
and marble-like pattern of the skin of her palms and feet. Clinical and instrumental examination
revealed no organic changes in the central nervous, cardiovascular, and respiratory systems. What
provisional diagnosis can be made?
13. A middle school teacher with 4-year-long record of work was issued a medical certificate for
pregnancy and childbirth leave. What amount of pay will she receive for the duration of her leave in
this case?
14. A 53-year-old man complains of general weakness, loss of appetite, and painful vesicles appearing
on his skin. The disease onset occurred suddenly, after hyperinsolation one week ago. Examination
detects isolated vesicles with wrinkled opercula and occasional painful erosions on the skin of the
patient’s torso and limbs. Nikolsky sign is positive. What is the most likely diagnosis?
Explanation
Nikolsky's sign has been a very useful diagnostic tool in cases of skin disorders like pemphigus, toxic epidermal necrolysis, etc., The sign is demonstrated when lateral pressure is applied on the border of an intact blister, which results in the dislodgment of the normal epidermis and extension of the blister. For the Nikolsky sign in patients with active blistering, firm sliding pressure with a finger separates normal-appearing epidermis, producing an erosion. This sign is made possible due to the loss of cell-to-cell adhesion in the epidermis.
Acantholysis is the loss of intercellular connections, such as desmosomes, resulting in loss of cohesion between keratinocytes, seen in diseases such as pemphigus vulgaris. It is absent in bullous pemphigoid, making it useful for differential diagnosis. Hence, Nikolsky’s sign will be negative in non-acantholytic pemphigus.
Nikolsky's sign is pathognomonic for pemphigus, toxic epidermal necrolysis, and staphylococcal scalded skin syndrome (SSSS). This sign basically differentiates intraepidermal blisters from subepidermal blisters.
Toxicoderma are usually caused by drugs and this patient has no history of taking any medication that would have resulted in toxicoderma. Dermatitis herpetiformis is an autoimmune blistering disorder associated with a gluten-sensitive enteropathy (patient wasn’t diagnosed of celiac disease). Herpes usually presents as grouped vesicles, meanwhile, on examination of the patient isolated vesicles were detected.
15. A 45-year-old woman came to the maternity clinic with complaints of periodical pains in her
mammary glands that start 1 day before menstruation and stop after the menstruation begins.
Palpation of the mammary glands detects diffuse nodes predominantly in the upper outer
quadrants. What is the most likely diagnosis?
16. A 48-year-old woman developed insomnia, depressive mood, anxiety, fears and suicidal thoughts
after the death of her husband that occurred one month ago. During her stay in the hospital she
speaks in a low voice, is depressed, anxious, avoids sleeping, refuses to eat. What medications
should be prescribed in this case?
17. A 22-day-old infant developed subcutaneous red nodes from 1.0 to 1.5 cm in size on the scalp;
later the nodes suppurated. Temperature increased up to 37.70C, intoxication symptoms appeared,
regional lymph nodes enlarged. Complete blood count: anemia, leukocytosis, neutrocytosis,
increased ESR. What diagnosis can be made?
18. The 5-year-old child has been ill for 2 weeks. Cough attacks developed first and were then followed
by reprises. During coughing the child’s face turns red and cervical veins bulge. The cough attacks
induce vomiting. X- ray shows intensified bronchial pattern. Blood test: leukocytes - 16∙109/L ,
lymphocytes - 72%, erythrocyte sedimentation rate - 4 mm/hour. What is the most likely diagnosis?
19. A woman has been provisionally diagnosed with pheochromocytoma. At the stage of intermission
her BP is within norm; there is a tendency towards tachycardia. No urine pathologies. The decision
has been made to perform a provocative test with histamine. What drug should be kept close at
hand for emergency aid in case of positive test result?
20. A 46-year-old woman came to the maternity clinic with complaints of moderate blood discharge
from the vagina, which developed after the menstruation delay of 1.5 months. On vaginal
examination: the cervix is clean; the uterus is not enlarged, mobile, painless; appendages without
changes. Make the diagnosis:
21. In the inpatient gynecological unit within a year 6500 women underwent treatment. They spent
there a total of 102000 bed-days. What indicator of the gynecological unit work can be calculated
based on these data?
22. A 52-year-old man for the last 3 years has been suffering from difficult swallowing of solid food,
burning retrosternal pain that aggravated during eating, loss of body mass, and occasional vomiting
with undigested food. Esophageal X-ray shows S-shaped deformation of the esophagus and its
dilation; at the cardiac orifice the esophagus is constricted; esophageal mucosa is smooth, without
signs of peristalsis. Make the provisional diagnosis:
23. A woman is 40 weeks pregnant. The fetus is in the longitudinal lie and cephalic presentation. Pelvic
size: 26-29-31-20. Expected weight of the fetus is 4800 gram. The labor contractions has been
lasting for 12 hours, within the last 2 hours they were extremely painful, the parturient woman is
anxious. The waters broke 4 hours ago. On external examination the contraction ring is located 2
finger widths above the navel, Henkel-Vasten sign is positive. Fetal heart rate is 160/min., muffled.
On internal examination the uterine cervix is fully open, the head is engaged and pressed to the
entrance into the lesser pelvis. What is the most likely diagnosis?
24. At the railroad crossing a passenger train collided with a bus. In this collision 26 bus passenges
died, another 18 passengers received mechanical injuries of varying severity. Where will be
professional medical aid provided for the victims of this accident? Who will provide this aid?
25. A 6-month-old child on breastfeeding is hospitalized in the inpatient department. After the child
recovers, the doctor recommends the mother to start introducing solid food to the child’s diet. What
products should be introduced to the child’s diet first?
26. A surgery unit received a person with an incised stab wound on the upper third of the right thigh.
Examination detects an incised stab wound 3.0x0.5x2.0 cm in size on the inner surface of the
upper third of the right thigh. Bright-red blood flows from deep within the wound in a pulsing stream.
Characterize this type of bleeding:
27. A 38-year-old patient has been brought by an ambulance to the surgical department with
complaints of general weakness, indisposition, black stool. On examination the patient is pale,
there are dotted hemorrhages on the skin of his torso and extremities. On digital investigation there
are black feces on the glove. Blood test: Hb - 108 g/L, thrombocytopenia. Anamnesis states that a
similar condition was observed 1 year ago. Make the diagnosis:
28. A 23-year-old man complains of severe pain in his left knee joint. Objectively the left knee joint is
enlarged, with hyperemic skin, painful on palpation. Complete blood count: erythrocytes -
3.8∙1012/L, Hb - 122 g/L, leukocytes - 7.4∙109/L, platelets - 183∙109/L. Erythrocyte sedimentation
rate - 10 mm/hour. Bleeding time (Duke method) - 4 min., Lee-White coagulation time - 24 min.
Partial thromboplastin time (activated) - 89 seconds. Rheumatoid factor - negative. What is the
most likely diagnosis?
29. A 42-year-old man, a dispatcher, suffes from peptic ulcer disease of the duodenum. The disease is
of moderate severity. He wants to be assigned a disability group. Make the conclusion regarding his
working ability:
30. A 16-year-old girl has primary amenorrhea, no pubic hair growth, normally developed mammary
glands; her genotype is 46 XY; uterus and vagina are absent. What is your diagnosis?
31. A 72-year-old man diagnosed with ischemic heart disease presents with diffuse cardiosclerosis,
permanent tachysystolic atrial fibrillation, heart failure IIa, FC III. Objective examination of vital
signs: blood pressure is 135/80 mm Hg, heart rate is 160/min., pulse is 125/min. Left ventricular
ejection fraction is 32%. What drug is indicated in this case and should be presribed to the patient?
32. A 32-year-old woman complains of tumor-like formation on the anterior surface of her neck that
appeared 2 years ago. Within the last 3 months the tumor has been rapidly growing. It hinders
swallowing and impairs speech; the tumor causes a sensation of pressure. Objectively the skin
moisture is normal, pulse is 80/min., rhythmic, blood pressure is 130/80 mm Hg. In the right lobe of
the thyroid gland there is a dense lumpy node 3.0x3.5 cm that moves during swallowing. Scanning
image shows a ”cold nodule” in the thyroid gland. Make the provisional diagnosis:
33. A 17-year-old girl has made an appointment with the doctor. She plans to begin her sex life. No
signs of gynecological pathology were detected. In the family history the patient’s grandmother had
cervical cancer. The patient was consulted about the maintenance of her reproductive health. What
recommendation will be the most helpful for prevention of invasive cervical cancer?
34. In the air of the feed kitchen at the poultry factory, at the area where formula feed is being mixed,
the dust concentration reaches 200 mg/m3. Air microflora is represented predominantly by
Asperqillus and Mucor fungi. What effect determines pathogenic properties of the dust?
35. A 32-year-old woman complains of body weight loss despite her increased appetite, nervousness,
and tremor of the extremities. Objectively: the skin is moist; the thyroid gland is diffusely enlarged,
painless, soft, and mobile. Blood test: increased level of T3, T4, and thyroid-stimulating hormone
(THS). What is the most likely diagnosis?
Explanation
Diffuse toxic goiter or grave’s disease is an autoimmune disease characterised by an increased amount of thyroid hormones ( T3- triiodothyronine and T4- thyroxine). Symptoms include; loss of weight, with increased appetite, increased sweating, cardiac findings (tachycardia, increased risk for atrial fibrillation), tremors of extremities, heat intolerance, diarrhea, anxiety etc.
It is the most common cause of hyperthyroidism and more common in females than males. There is production of IgG antibodies against the TSH receptor (stimulating type of antibody - Type II hypersensitivity reaction)
Hashimoto’s thyroiditis is a destructive autoimmune thyroiditis leading to hypothyroidism.
In Diffuse non-toxic goiter, thyroid function is normal and patients are often asymptomatic. It manifests without hyperthyroidism, hypothyroidism, or inflammation.
36. A 78-year-old man with a prostate adenoma underwent a herniotomy for a direct inguinal hernia.
After the surgery he presents with absent urination. Enlarged urinary bladder is detectable above
the patient’s pubis. What measures should be taken in this case?
37. An 11-year-old boy for a month has been presenting with increasing pain in the right femur. In the
painful area there is a non- mobile painful tumor with unclear margins. The child complains of
general indisposition, weakness, increased body temperature up to 39°C. X-ray shows widened
medullary cavity, small foci of cancellous bone destruction, and onion-like lamellar exfoliation of the
cortical layer. What is the most likely pathology resulting in such clinical presentation?
Explanation
Ewing's sarcoma typically occurs in children and young adults. Symptoms include pain, swelling and fever.
Ewing sarcoma is cancer that occurs primarily in the bone or soft tissue. While Ewing sarcoma can develop in any bone, it is most often found in the hip bones, ribs, or long bones (e.g., femur (thighbone), tibia (shinbone) or humerus (upper arm bone)). It can involve the muscle and the soft tissues around the tumor as well. Ewing sarcoma cells can also metastasize (spread) to other areas of the body, including the bone marrow, lungs, kidneys, heart, adrenal glands and other soft tissues.
Findings on imaging:
-
lesion may be purely lytic or have variable amounts of reactive new bone formation
-
periosteal reaction may give “onion skin” or “sunburst” appearance
-
large destructive lesion in the diaphysis or metaphysis with a permeative moth eaten appearance.
38. A 45-year-old man, a farmer, presents with acute onset of a disease. He complains of headache,
high temperature, pain in the gastrocnemius muscles, icteric face, and dark urine. Objectively: body
temperature - 38°C, blood pressure - 100/70 mm Hg, conjunctival hemorrhages,
hepatosplenomegaly, and oliguria. What is the most likely provisional diagnosis?
Explanation
Leptospirosis is an acute generalized infectious disease, characterized by extensive vasculitis, caused by spirochetes of the genus Leptospira. It presents with flu-like symptoms, myalgias (majorly calf muscles eg gastrocnemius), jaundice (icteric face), Photophobia etc. The icterohemorrhagic form of leptospirosis presents with a severe form of jaundice and azotemia from the liver and kidney dysfunction coupled with anemia. Leptospira is commonly found in water contaminated with animal urine.
N/B Virus hepatitis has a gradual onset, without chills, the temperature rises at the pre-icteric period. Muscle pains, scleritis, conjunctivitis are not characteristic of it.
Brucellosis is caused by gram negative bacteria, transmitted via ingestion of contaminated animal products (eg, unpasteurized milk). Typically presents with fever, night sweats, and arthralgia but jaundice is usually absent.
39. During medical examination of high and middle school students, the doctors vere assessing
correlation between biological and calendar age of the school students based on the following
criteria: height growth rate per year, ossification of the carpal bones, the number of permanent
teeth. What additional development criterion should be assessed at this age?
Explanation
Most students in high school are 10 - 11 years and above. Development of secondary sexual characteristics begins in puberty, therefore it should be considered when considering the biological age of high and middle school students.
There are two types of physical changes that occur during puberty: a) changes to primary sex characteristics and b) changes to secondary sex characteristics. Primary sex characteristics refer to changes to the sexual organs themselves (uterus, vagina, penis, and testes). Secondary sex characteristics refer to other visible changes that mark adult maturation such as changes in height and body shape.
For males, secondary characteristics include facial and chest hair, increased body hair, pelvic build (lack of rounded hips), upper body muscular build, and the ability to generate muscle mass at a faster rate than the female. For females, secondary sex characteristics include relative lack of body hair, thicker hair on the head (in some cases), rounded hips/figure, a decreased ability to generate muscle mass at a fast rate, decreased upper body strength, breasts, ability to nurse children, a menstrual cycle, and increased body fat composition.
Tanner staging is a very helpful tool in determining the stage of secondary sex characteristic development.
40. A 3-week-old infant developed large, flaccid vesicles with purulent contents on the skin of chest and
abdomen. The vesicles rupture quickly. Make the provisional diagnosis:
Explanation
Pemphigus Neonatorum is a disease of the newborn, in which vesicles or blebs, usually flat on the top, appear with or without fever, on a perfectly normal or reddened skin with pin-head size vesicle elevation, which rapidly develops into a large bleb. As the disease progresses, relapses may occur, yet the infant may recover promptly after a single outbreak of but few blebs. In some cases these blebs show a marked tendency to peripheral extension, which finally dry, leaving a thin brown crust. Staphylococcus aureus have been implicated as the causative agent.
The distinction between Pemphigus and syphilis in the newborn may be determined by the localization of the eruption. Syphilis will be localized to the palms of the hands and soles of the feet, as well as by the associating symptoms of syphilis.
Vesiculo Pustulosis is also a disease of the newborn, characterized by multiple pustules, emerging in the openings of ducts of eccrine sweat glands. In pathogenesis the main role is played by maceration of the skin, prematurity, artificial feeding. Localization - skin of butttocks, hips, inguinal folds, head etc.
Erythema toxicum occurs more often in term babies of multigravidas. It usually arises in the first 4 days of life and fades within 4 days. Occasionally onset is delayed until 10 days after birth or it recurs in the first 2–6 weeks after birth. It is characterised by red macules and papules, with pustules appearing in a third of cases.
41. A 42-year-old man, a worker at the meat processing factory, developed an itching spot on his lower
jaw, which gradually transformed into a slightly painful carbuncle 3 cm in diameter, surrounded by a
painless swelling that reaches the clavicle. Temperature is subfebrile, under 37.8°C. The doctor
suspects anthrax. What drug should this man be prescribed for treatment?
Explanation
Bacillus anthracis is an aerobic, non-motile, spore forming, large non-hemolytic Gram-positive rod that grows well on blood agar. The clinical manifestations of human anthrax - Cutaneous and Inhalation.
Cutaneous anthrax, the most common form of naturally occurring disease, begins as a small, painless, pruritic papule that within 2 days enlarges, develops vesicles, and ulcerates to form an eschar. Inhalational anthrax follows inhalation of infectious doses of anthrax spores.
Four antibiotics are approved for use for post exposure prophylaxis following exposure to aerosolized spores of B. anthracis: doxycycline, ciprofloxacin, levofloxacin, and parenteral procaine penicillin G. Of all these four antibiotics, only Penicillin is listed as a choice for this question.
42. A child is 1 year old. After solid food was introduced into the diet, within the last several months the
child developed loss of appetite, diarrhea with large amount of feces, and occasional vomiting.
Body temperature remains normal. Body weight is 7 kg. The child is very pale, has leg edemas and
extremely distended abdomen. Feces analysis detects high levels of fatty acids and soaps.
Diagnosis of celiac disease was made and gluten-free diet was prescribed. What should be
excluded from the diet in this case?
Explanation
Celiac disease is an immune reaction to eating gluten, a protein found in wheat, barley and rye. Sometimes called celiac sprue or gluten-sensitive enteropathy. When people with celiac disease eat gluten (a protein found in wheat, rye and barley), their body mounts an immune response that attacks the small intestine. These attacks lead to damage on the villi, small fingerlike projections that line the small intestine, that promote nutrient absorption. When the villi get damaged, nutrients cannot be absorbed properly into the body.
Celiac disease is hereditary, meaning that it runs in families. People with a first-degree relative with celiac disease (parent, child, sibling) have a 1 in 10 risk of developing celiac disease.
Celiac disease can develop at any age after people start eating foods or medicines that contain gluten.
Oats contain avenin, which is a protein similar to gluten. Research has shown that most people with coeliac disease can tolerate gluten free oats with no problems. The issue is that sometimes oats are produced in the same place as wheat, barley and rye, and then become contaminated with these other grains.
43. A patient is being treated in the tuberculosis clinic. Throughout the last 3 weeks he has been
suffering from headaches of increasing intensity. Neurological examination detects nuchal rigidity
without focal signs. Make the provisional diagnosis:
44. A 37-year-old man suddenly developed acute headache accompanied by nausea, vomiting, and
impaired consciousness. Objectively blood pressure is 190/120 mm Hg, the face is hyperemic.
Patient’s consciousness is clouded, his answers to the questions are short, monosyllabic.
Movement and sensory disturbances are absent. Meningeal signs are positive. Cerebrospinal fluid
contains blood. What provisional diagnosis can be made?
45. A 20-year-old student after failing an exam developed complaints of a sensation of a round foreign
body in her throat, difficult swallowing. She fixates on her condition, limits her diet, often cries,
seeks attention, exhibits demonstrative attitude. She is highly susceptible to psychotherapeutic
suggestion. What psychiatric diagnosis can be made in this case?
46. Employees work in conditions of high dust concentration. Certain chemical (silicon dioxide content)
and physical properties of dust aerosols contribute to the development of occupational dust-
induced diseases. What is the main physical property of dust aerosols?
47. A 32-year-old man complains of pain in his legs that intensifies during walking, intermittent
claudication, numbness of his toes, extremity coldness, and inability to walk more that 100 meters.
When he sleeps, his leg usually hangs down. The patient has been smoking since he was 16. He
drinks alcohol in excess. The left leg is colder than the right one; the skin of the extremities is dry.
No pulse can be detected on the pedal arteries, while pulsation of the femoral arteries is retained.
What is the most likely diagnosis?
Explanation
Obliterating Endarteritis is also known as Buerger’s disease and vasculitis. The condition is thought to occur as a result of tobacco use and more common in males. The disease is characterized by inflammation and thrombosis of small and medium arteries of the legs and feet which recurs and progresses in stages. During the ischemic period, the veins of the lower leg are inflamed, skin has ulceration, and there is gangrene with intermittent claudication. During the nutritional disorder period there is persistent pain and muscle atrophy. During the necrosis period, the pain becomes worse as infection leads to the development of ulcers and gangrene. Pains usually persist; In addition, the patient usually complains of coldness and numbness. Burning sensations is another disturbing symptom.
Treatment usually has to do with smoking cessation.
Raynaud disease is a condition in which some areas of the body feel numb and cool in certain circumstances. In Raynaud's phenomenon, smaller arteries that supply blood to the skin constrict excessively in response to cold, limiting blood supply to the affected area. The fingers, toes, ears and tip of the nose are commonly involved and feel numb and cool in response to cold temperatures or stress.
Leriche Syndrome, also commonly referred to as aortoiliac occlusive disease, is a product of atherosclerosis affecting the distal abdominal aorta, iliac arteries, and femoropopliteal vessels.
48. A 10-year-old boy with symptoms of arthritis and myocarditis was brought to a hospital. Based on
clinical examination the provisional diagnosis of juvenile rheumatoid arthritis was made. What
symptom is the most contributive for the diagnostics of this disease?
49. A 39-year-old man suffers from chronic rheumatic heart disease. He complains of dyspnea during
physical exertion, cough with expectoration, and palpitations. Auscultation detects intensified I heart
sound and diastolic murmur; the sound of opening mitral valve can be auscultated at the cardiac
apex. The II heart sound is accentuated over the pulmonary artery. The patient is cyanotic. X-ray
shows dilated pulmonary root and enlargement of the right ventricle and left atrium. What is the
most likely diagnosis?
Explanation
|
Valvular diseases
|
Mitral stenosis
|
Aortic stenosis
|
Aortic regurgitation
|
Mitral regurgitation
|
Tricuspid regurgitation
|
|
Main causes and risk factors
|
Almost always caused by rheumatic heart disease
|
-Calcification of tricuspid aortic valve with age
(>50%)
-Calcification of bicuspid aortic valve
(30-40%)
-Rheumatic fever
(<10%)
Hypertension, diabetes mellitus, hyperlipoproteinemia and uremia may speed up the process.
|
Acute
-Infective endocarditis
-Trauma
Chronic
-Primary valvular: rheumatic fever, bicuspid aortic valve, Marfan's syndrome, Ehlers–Danlos syndrome, ankylosing spondylitis, systemic lupus erythematosus
-Disease of the aortic root: syphilitic aortitis, osteogenesis imperfecta, aortic dissection, Behçet's disease, reactive arthritis, systemic hypertension
|
Acute
-Endocarditis, mainly S. aureus
-Papillary muscle rupture or dysfunction, including mitral valve prolapse
Chronic
-Rheumatic fever
-Marfan's syndrome
-Cardiomyopathy
|
Usually secondary to right ventricular dilation
Other causes: Tricuspid endocarditis, rheumatic fever, Ebstein's anomaly, carcinoid syndrome and myxomatous degeneration
|
|
Symptoms
|
Heart failure symptoms, such as dyspnea on exertion, orthopnea and paroxysmal nocturnal dyspnea
-Palpitations
-Chest pain
-Hemoptysis
-Thromboembolism
-Ascites and edema (if right-sided heart failure develops)
Symptoms increase with exercise and pregnancy
|
-Heart failure symptoms, such as dyspnea on exertion (most frequent symptom), orthopnea and paroxysmal nocturnal dyspnea
-Angina pectoris
-Syncope, usually exertional
|
-Heart failure symptoms, such as dyspnea on exertion, orthopnea and paroxysmal nocturnal dyspnea
Palpitations,
-Angina pectoris
-In acute cases: cyanosis and circulatory shock
|
-Heart failure symptoms, such as dyspnea on exertion, orthopnea and paroxysmal nocturnal dyspnea
-Palpitations
-Pulmonary edema
|
Symptoms of right-sided heart failure, such as ascites, hepatomegaly, edema and jugular venous distension
|
|
Medical signs
|
-Opening snap followed by a low-pitched diastolic rumble with presystolic accentuation.
The opening snap follows closer to the S2 heart tone with worsening stenosis.
The murmur is heard best with the bell of the stethoscope lying on the left side and its duration increases with worsening disease.
-Loud S1 - may be the most prominent sign
-Advanced disease may present with signs of right-sided heart failure such as parasternal heave, jugular venous distension, hepatomegaly, ascites and/or pulmonary hypertension (presenting with a loud P2.
Signs increase with exercise and pregnancy
|
Systolic murmur of a harsh crescendo-decrescendo type, heard in 2nd right intercostal space, radiating to the carotid arteries
-Pulsus parvus et tardus, that is, diminished and delayed carotid pulse
-Fourth heart sound
-Decreased A2 sound
-Sustained apex beat
Precordial thrill
|
-Increased pulse pressure by increased systolic and decreased diastolic blood pressure, but may not be significant if acute
-Diastolic decrescendo murmur best heard at left sternal border
Water hammer pulse
-Austin Flint murmur
-Apex beat displaced down and to the left
-Third heart sound may be present
|
Holosystolic murmur at the apex, radiating to the back or clavicular area
Commonly atrial fibrillation
Third heart sound
Laterally displaced apex beat, often with heave
Loud, palpable P2, heard best when lying on the left side
|
-Pulsatile liver
-Prominent V waves and rapid descents in jugular venous pressure
-Inspiratory third heart sound at left lower sternal border (LLSB)
-Blowing holosystolic murmur at LLSB, intensifying with inspiration, and decreasing with expiration and -Valsalva maneuver
-Parasternal heave along LLSB
-Atrial fibrillation is usually present
|
50. A 14-year-old girl came to the general practitioner with complaints of weakness, loss of appetite,
headache, rapid fatigability. Her last menstruation was profuse and lasted for 14 days after the
previous delay of 2 months. Objectively: the skin is pale, heart rate is 90/min., BP is 110/70 mm Hg,
Hb is 88 g/L. Rectal examination: the uterus and its appendages are without changes, no discharge
from the genital tracts. What complication occurred in the patient?
51. An 18-year-old young man complains of pain in his knee and elbow joints and body temperature up
to 39.5°C. One week and a half earlier he developed sore throat. On examination his body
temperature is 38.5°C. Swelling of the knee and elbow joints is observed. Pulse is 106/min..
rhythmic. Blood pressure is 90/60 mm Hg. Cardiac borders are unchanged, heart sounds are
weakened, at the cardiac apex there is a soft systolic murmur. What factor would be the most
indicative of the likely disease etiology?
52. A woman undergoing in-patient treatment for viral hepatitis type B developed headache, nausea,
recurrent vomiting, memory lapses, flapping tremor of her hands, and rapid pulse. Sweet smell from
her mouth is detected. Body temperature is 37.6°C, heart rate is 89/min. What complication
developed in the patient?
Explanation
Acute liver failure is a state of hepatic cells dysfunction, caused by unknown earlier liver disease, resulting in general intoxication, coagulation violations, neurological and mental disorders. Its etiology is usually connected with: viral hepatitis (hepatitis B virus, hepatitis A virus), poisonings (mushrooms, dichloroethane, phosphorus, carbon tetrachloride, arsenic), eclampsia, burn disease, anaesthetic gas, antibiotics, sulfanilamides, massive bacterial pneumonia, cirrhosis, hepatic tumours and metastasis.
Advanced liver failure manifests in a coma. The patient in question presents with viral hepatitis B (the probable cause of the liver failure) and a list of other symptoms which indicate neurological and intoxication disorder.
53. A 56-year-old woman was diagnosed with stage 2 hypertension of the 2nd degree. She belongs to
the group of moderate risk and has bronchial asthma. What group of drugs is CONTRAINDICATED
to this patient?
Explanation
Beta Blockers include: Atenolol, Bisoprolol, Carvedilol, Labetalol, Metoprolol, Propranolol etc (they end with ‘lol’).
They are effective as antihypertensives because they decrease cardiac output and also decrease renin secretion (due to Beta 1 receptor blockade on Juxtaglomerular cells in the Kidney).
However, they can also cause Asthma/COPD exacerbations; Erectile dysfunction; bradycardia or AV block.
Hence, this group of medications are contraindicated in patients with Bronchial Asthma.
Bronchial Asthma/COPD are pathological states associated with bronchoconstriction. In physiological states, when Beta 2 receptors in the bronchi are stimulated, they result in bronchodilation. So, when a Beta blocker is administered, it will result in Bronchoconstriction thereby exacerbating bronchial asthma in this patient.
54. A newborn girl has Apgar score of 7-8 points at the 1-5 minutes after birth. During the labor there
was a brief difficulty with extraction of the shoulder girdle. After birth the baby presents with
disturbed function of the proximal segment and forced position of the right arm. The shoulder is
rotated inwards, the elbow is extended, the forearm is pronated, and the whole upper limb
resembles an arm of a doll. What is the most likely clinical diagnosis in this case?
55. A 13-year-old girl for a month has been complaining of fatigability, dull pain in her right subcostal
area, abdominal distension, and constipations. Abdominal palpation reveals positive Kehr, Murphy,
and Ortner signs, while Desjardins and Mayo-Robson points are painless. Total bilirubin is 14.7
mcmol/L, predominantly indirect, ALT - 20 U/L, AST - 40 U/L, amylase - 6.3 mmol/L.
Echocholecystography shows practically no contraction of the gallbladder. Make the provisional
diagnosis:
56. During examination a 4-month-old child with meningococcemia presents with acrocyanosis, cold
extremities, tachypnea, and thready pulse, blood pressure of 30/0 mm Hg, anuria, and sopor. What
clinical syndrome is it?
57. A 25-year-old woman has been suffering from diabetes mellitus since she was 9. She was admitted
into the nephrology unit with significant edemas of the face, arms, and legs. Blood pressure -
200/110 mm Hg, Hb - 90 g/L, blood creatinine - 850 mcmol/L, urine proteins - 1.0 g/L, leukocytes -
10-15 in the vision field. Glomerular filtration rate - 10 mL/min. What tactics should the doctor
choose?
58. During regular medical examination a lyceum student presents with signs of cheilitis that manifests
as epithelial maceration in the area of lip seal. The lips are bright-red, with single vertical cracks
covered with brown- red scabs. These clinical signs are most likely caused by insufficient content of
the following in the diet:
59. A 34-year-old man on the 3rd day of ceftriaxone treatment for acute otitis (daily dosage - 2 grams)
developed diarrhea occurring 5-6 times per day. Feces are without mucus or blood admixtures.
Temperature is 36.6°C. Gregersen reaction (occult blood in feces) is negative. Stool culture
detected no pathogenic germs. What is the most likely cause of diarrhea in this case?
60. A 13-year-old girl has 30% of excessive body mass, she started to gain weight at the age of 3. She
has a family history of obesity. Her height and sexual development are normal for her age. The
appetite is excessive. She complains of periodical headaches. Blood pressure - 120/80 mm Hg.
Subcutaneous fat is evenly distributed, she has no stretch marks. There is juvenile acne on her
face. What type of obesity is it?
61. Disease onset was acute. A child developed general weakness, pain in the joints, and elevated
temperature. Later these signs became accompanied by itching skin rash manifested as
erythematous spots 2- 5 mm in size. The rash gradually turned hemorrhagic. Large joints are
painful and swollen; pain attacks periodically occur in the paraumbilical area; there are signs of
intestinal hemorrhage. What is the most likely diagnosis?
Explanation
Henoch-Schönlein purpura (HSP) is an acute immunoglobulin A (IgA)–mediated disorder characterized by a generalized vasculitis involving the small vessels of the skin, the gastrointestinal (GI) tract, the kidneys, the joints, and, rarely, the lungs and the central nervous system (CNS).
It is a disease involving inflammation of small blood vessels. It most commonly occurs in children. The main symptom is a rash with numerous small bruises, which have a raised appearance, over the legs or buttocks.
It is characterized by a triad of palpable purpura (without thrombocytopenia), abdominal pain, and arthritis. In the skin, the disease causes palpable purpura (small, raised areas of bleeding underneath the skin), often with joint pain and abdominal pain. With kidney involvement, there may be a loss of small amounts of blood and protein in the urine (hematuria and proteinuria), but this usually goes unnoticed; in a small proportion of cases, the kidney involvement proceeds to chronic kidney disease. HSP is often preceded by an infection, such as a throat infection.
62. Clinical trials have proved the ”Lipoflavon” drug to be effective for treatment of unstable angina
pectoris in the control group and experimental group of patients. Neither patients nor researchers
knew who belonged to which group. Name this type of study:
63. A 26-year-old man complains of chills, rhinitis, dry cough, and fever up to 38°C. Examination shows
him to be in a moderately severe condition; there are small pale pink non-merging spots on the skin
of his back, abdomen, and extremities. Palpation reveals enlarged occipital and axillary lymph
nodes. No information about vaccination history could be obtained. What is the likely etiology of this
disease?
Explanation
Rubella (caused by rubella virus) is an acute viral infection characterised by a short prodromal period, Exanthema ( rash) during three days and lymphadenopathy. The type of rash found is roseola and small maculo-papula. Note that the rash elements do not merge (non-merging spots) and are usually concentrated on the extensor surface of extremities, back, buttocks and outer surface of thigh. Commonly associated with enlarged occipital lymph nodes.
Epstein-barr virus is one of the causative agents of Infectious mononucleosis- a disease characterised by prolonged fever, systemic lymphadenopathy,acute tonsillitis, acute adenoiditis, hepatosplenomegaly, along with typical blood changes such as lymphocytosis, monocytosis, presence of specific cells called atypical mononuclear cells or virocytes.
Mumps infection is a systemic disease characterised by hyperthermic syndrome, symmetrical or unilateral swelling of parotid glands, epididymo-orchitis etc.
64. A 3-year-old child presents with dyspnea that abates in the sitting position, occasional loss of
consciousness and seizures, delayed physical development, cyanosis, drumstick fingers.
Echocardioscopy detects aortic dextraposition, ventricular septal defect, pulmonary artery stenosis,
and right ventricular hypertrophy. What is the most likely diagnosis?
65. A 55-year-old woman complains of pain and popping sounds in her left knee joint, which occur
when she climbs the stairs. Occasionally during movements her joint becomes ”stuck”. 5 years ago
she suffered a trauma of her left knee. Complete blood count and biochemical blood analysis show
normal results. X-ray shows marked osteosclerosis and osteophytes. The joint space is narrowed.
Make the provisional diagnosis:
66. A 16-year-old patient has made an appointment with an otolaryngologist. He complains of elevated
body temperature and sore throat. Disease onset was 2 days ago, after the patient ate two portions
of ice-cream. Pharyngoscopy shows hyperemic mucosa of the palatine tonsils, with purulent
exudate in the lacunae. Make the provisional diagnosis:
Explanation
Tonsillitis is a generalized infectious disease with inflammation of the pharyngeal lymphoid structures, and with swelling of the regional lymphatic glands. The cause of tonsillitis is invasion by streptococci and, less frequently, by staphylocci and pneumococci.
Tonsillitis may occur in the catarrhal, lacunar and follicular forms.
In lacunar tonsillitis the general symptoms are more pronounced, more severe than in catarrhal tonsillitis, with pain on swallowing, sometimes radiates to the ear, headache, fever as high as 40 °C. The disease often disappears on the fourth or fifth day.
A continuous coat made up of yellowish-white membranes or patches often covers the free surface of the tonsils without extending beyond their limits (doesn’t extend beyond the lacunae or crypts). In lacunar tonsillitis the formation of patches in the lacunar openings distinguishes this disease from diphtheria.
Take note of this statement in the question stem:
Pharyngoscopy shows hyperemic mucosa of the palatine tonsils, with purulent exudate in the lacunae.
67. A 10-year-old girl exhibits high level of physical development (M + 3σ), her body length increased
by 10 cm within a year (which is double the norm for her age group), the number of permanent
teeth corresponds with the age norm (20), the development of her secondary sex characteristics is
three years ahead of her age (Ma, P, Ax, Menarche). Development rate ahead of her biological age
can occur due to:
68. A 30-year-old woman came to the gynecological department. She complains of sharp pain in her
lower abdomen and temperature of 38.8°C. She has a history of extramarital sexual activity and 2
artificial abortions. On gynecological examination the uterus is unchanged. The appendages are
bilaterally enlarged and painful. Profuse purulent discharge is being produced from the vagina.
What examination needs to be conducted to clarify the diagnosis?
69. A 27-year-old woman complains of foul-smelling discharge from her genital tracts, pain in her lower
abdomen, and elevated temperature. The complaints arose 2 days ago. She has a history of
surgical abortion at the term of 8 weeks one week ago. Mirror examination: the uterine cervix is
clear, external orifice produces foul-smelling discharge. Vaginal examination: the uterus lies in
anteflexion, is mobile, painful, and slightly enlarged. The appendages are without changes. Make
the provisional diagnosis:
Explanation
Look closely at the clue given in the question, the patient had abortion a week ago then the symptoms listed above started. This is a clear pointer to a post-abortion complication.
You’re at risk of getting an infection that can cause endometritis after a miscarriage or after childbirth, especially following a long labor or a cesarean delivery. You’re also more likely to get endometritis after a medical procedure that involves entering the uterus through the cervix. This can provide a pathway for bacteria to enter. Medical procedures that can increase your risk of developing endometritis include: hysteroscopy, placement of an intrauterine device, dilation and curettage (uterine scraping).
Endometritis is an inflammatory condition of the lining of the uterus and is usually due to an infection. It’s usually not life-threatening, but it’s important to get it treated as soon as possible. Endometritis typically causes the following symptoms: abdominal swelling, abnormal vaginal bleeding, abnormal vaginal discharge, fever, general feeling of sickness, pain in the pelvis, lower abdominal area, or rectal area.
In this scenario, the patient had a surgical abortion and this procedure most likely introduced the infection into the patient.
Appendicitis is often characterized by right iliac fossa tenderness. From the question, the appendages are without changes, so we can rule out salpingoophoritis (inflammation of the fallopian tube and ovaries). This has nothing to do with the respiratory system (acute respiratory disease) or colon (enterocolitis).
70. A 2-year-old child with persisting cough and subfebrile body temperature after a case of URTI
developed dyspnea, cyanosis of the nasolabial triangle, percussion dullness and weakened
respiration in the lower lobe of the right lung, and a slight mediastinal displacement to the left. What
pulmonary pathology is likely to cause this clinical presentation?
Explanation
When you breathe, the thin tissues that line your lungs and chest wall, called the pleura, rub together. Typically, this isn’t a problem because the tissue is satiny and generates no friction. However, when this tissue is inflamed or infected, it becomes irritated and swollen, causing significant pain. This condition is known as pleurisy or pleuritis.
Viral infections are the most common cause of pleurisy which is suspected in this case with a subfebrile temperature in a patient with Upper Respiratory Tract Infection (URTI). Bacteria, heart surgery complications, autoimmune disorders, trauma could also cause pleurisy.
The chief symptom associated with pleurisy is a sharp, stabbing pain when you breathe. This pain often limits respiratory excursions on the affected side thereby limiting gaseous exchange which can manifest as shallow breathing to avoid feeling pain, cyanosis and dyspnea.
Pleurisy can be accompanied by a fluid buildup that puts pressure on the lungs and causes them to stop working properly. This fluid accumulation is called a pleural effusion (percussion dullness on the right lower lung lobe). A person with a pleural effusion will eventually experience shortness of breath as the fluid increases.
71. A 58-year-old woman came to the gynecological clinic. She complains of bloody discharge from her
genital tracts. Menopause is 8 years. Gynecological examination: the uterus is slightly enlarged,
dense to touch, with limited mobility; the uterine appendages cannot be detected; parametrium is
free. Fractional curettage of the uterine cavity yields a significant amount of medullary substance in
the scrape. What is the most likely diagnosis?
72. A 59-year-old man complains of pain in his left eye and left side of his head, significant vision
impairment of the left eye, nausea, and vomiting. Visual acuity of the right eye is 1.0. Visual acuity
of the left eye is 0.03, attempts at correction bring no improvement. Right eye intraocular pressure -
21 mm Hg, left eye intraocular pressure - 65 mm Hg. Congestive injection is observed on the sclera
of the left eye. The cornea is thick and swollen. The anterior chamber is shallow, moist, and clear.
The pupil is dilated and unresponsive to the light, the fundus of the eye is not visible. What is the
most likely diagnosis?
Explanation
Glaucoma is a set of ocular disorders often defined by increased intraocular pressures leading to optic neuropathy and vision loss if untreated. Acute attack of glaucoma is caused by a rapid or sudden increase in pressure inside the eye, called intraocular pressure (IOP). Symptoms include - eye pain, severe headache, very blurry or hazy vision, redness in the white part of the affected eye, nausea or vomiting, sudden loss of sight etc.
The commonly accepted range for intraocular pressure is 10-22 mmHg (left eye is 65mmHg). Three factors that affect the intraocular pressure are the rate of production of aqueous humor by the ciliary body, the resistance to aqueous outflow through the trabecular meshwork and Schlemm’s canal, and the episcleral venous pressure.
The normal flow of aqueous humor starts in the ciliary body, goes through the pupil and out through the trabecular meshwork and Schlemm's canal in the angle of the anterior chamber. In acute angle-closure glaucoma, intraocular pressure increases rapidly due to outflow obstruction of the aqueous humor.
73. A 39-year-old man suffers from chronic adrenal insufficiency and receives replacement
glucocorticoid therapy (hydrocortisone - 15 mg/day). He is to undergo elective surgery for calculous
cholecystitis. What medication adjustment should be made on the day of the surgery to prevent the
development of acute adrenal insufficiency?
74. An 8-year-old girl complains of frequent painful urination in small amounts and urinary incontinence.
The signs have been present for 2 days already. She explains her disease by overexposure to cold.
Costovertebral angle tenderness is absent. Complete blood count is without pathologies. Urine test:
leukocytes - 20-30 in the vision field, erythrocytes - 40-50 in the vision field, unchanged, bacteriuria.
What is the most likely diagnosis?
75. A chronic alcoholic was hospitalized into the therapeutic inpatient unit due to pneumonia. On the
day 5 of his hospitalization he became disoriented in time and space, developed fear-inducing
visual hallucinations and motor agitation. Full body tremor and tremor of the limbs are observed. X-
ray and physical examinations detect the signs of his convalescence from pneumonia. What tactics
should be chosen regarding this patient?
76. During medical examination a cadet in the naval college was detected to have a painless dense
ulcer 1.5x0.5 in size in his perianal area at the 2 o’clock position. The ulcer floor resembles ”old fat”.
What is the provisional diagnosis?
77. A 52-year-old woman has been suffering for 2 years from dull, occasionally exacerbating pain in her
right subcostal area, occurring after eating high-fat foods, bitter taste in her mouth in the morning,
constipations, and flatulence. Objectively she has excess weight, her body temperature is 36.9°C;
there is a coating on the root of her tongue; the abdomen is moderately distended and painful in the
area of gallbladder projection. What examination would be the most helpful for diagnosis-making?
Explanation
From the question stem, the patient presents with symptoms indicating a gallbladder related issue (cholelithiasis, cholecystitis, cholangitis etc); these symptoms include: pain in the right subcostal area especially after eating food rich in fat, bitter taste in her mouth in the morning, constipations, and flatulence.
An ultrasound allows sonologists to view images of the organs and soft tissues inside your body. This procedure is used in diagnosing conditions related to the gallbladder. It is fast, accessible, not cumbersome and less expensive, which makes it a first choice in this case.
The other options are a bit cumbersome eg, Cholecystography requires use of contrast, and Duodenoscopy is more expensive.
78. In a rural health care area there is an increasing cervical cancer morbidity observed. The decision
is made to conduct a medical examination of the women living in this locality. What type of medical
examination is it?
79. A 45-year-old man diagnosed with acute pulmonary abscess suddenly developed sharp pain in his
chest on the right and dyspnea up to 30/min. Examination detects facial cyanosis and shallow rapid
respirations. Auscultation reveals acutely weakened respiration throughout the whole right lung;
percussion reveals a vesiculotympanitic (bandbox) resonance at the lung apex and dullness in the
lower lobe. What complication developed in this patient?
80. A 30-year-old multigravida has been in labour for 18 hours. 2 hours ago the pushing stage began.
Fetal heart rate is clear, rhythmic, 136/min. Vaginal examination reveals complete cervical
dilatation, the fetal head in the pelvic outlet plane. Sagittal suture is in line with obstetric conjugate,
the occipital fontanel is near the pubis. The patient has been diagnosed with primary uterine inertia.
What is the further tactics of labor management?
81. A 45-year-old man was brought by an ambulance into the emergency hospital. He complains of
sudden pain in the lumbar area, frequent painful urination, and vomiting. Examination detects pain
in the lumbar area, costovertebral angle tenderness, pain on palpation of kidneys and along the
ureter on the right. Urine test: proteins, fresh erythrocytes, leukocytes. Make the provisional
diagnosis:
82. A 26-year-old woman is suspected to suffer from systemic lupus erythematosus due to systemic
lesions of skin, vessels, joints, serous tunics, and heart that developed after photosensitization. The
following is detected: LE cells, antibodies to native DNA, isolated anti-centromere antibodies,
rheumatoid factor is 1:100, Wassermann reaction is positive, circulating immune complex is 120
units. What immunological indicators are considered to be specific to this disease?
83. A 40-year-old victim of a traffic accident sustained the following injuries: closed diaphyseal femur
fracture, brain concussion, multiple rib fractures, hemopneumothorax, degloving shin injuries. What
injuries require the most urgent attention?
Explanation
In resuscitating a patient, C-A-B sequence is very important.
C is to help maintain blood circulation; A - airway and B - Breathing.
Hemopneumothorax can be considered under these 3.
Hemo - active internal hemorrhage into the pleural cavity.
Pneumo - ongoing air leakage into the pleural cavity.
If these are not attended to first, eventually, the lungs will not be able to expand, hence, no gaseous exchange compromising both A- airway and B- breathing. If no action is taken, and the hemorrhage and air leakage into the pleural cavity continues, it will eventually lead to hypovolemia and the accumulated blood will compress the mediastinum which houses the heart thereby preventing the heart from contracting as well and eventually compromises C- circulation. Once this is attended to, the other injuries can receive proper care as well but hemopneumothorax comes first.
Now, considering this patient, there is no active external bleeding going on. Closed diaphyseal femur fracture just needs immobilization as first aid. It is not open and the question did not state that there is an injury to a major blood vessel. In Degloving shin injuries, if there is an active bleeding, the vessel can be ligated and the wound dressed.
The most common and least serious type of traumatic brain injury is called a concussion. A concussion is most often caused by a sudden direct blow or bump to the head.
84. A 36-year-old man complains of marked dyspnea and cardiac pain. He ascribes his disease to the
case of influenza that he had 2 weeks ago. Objectively he leans forward when sitting. The face is
swollen, cyanotic, cervical veins are distended. Heart borders are extended on the both sides, heart
sounds are muffled, heart rate = Ps = 118/min., BP is 90/60 mm Hg. Blood test: ESR is 46
mm/hour. ECG shows low voltage. X-ray shows trapezoidal cardiac silhouette and signs of
pulmonary congestion. Choose the treatment tactics:
85. Increased general morbidity of the local population is observed in the area near a factory, where
atmosphere is being intensively polluted with sulfurous gas. What effect does polluted air have on
human body in this case?
86. Heart X-ray of a 31-year-old man has revealed the following: with tightly filled opacified esophagus
there is a marginal filling defect in its middle third on the posterior wall; the defect is 1.8xl.3 cm in
size with clear oval border. Mucosal folds are retained and envelop the defect; wall peristalsis and
elasticity are not affected. There are no complaints regarding the condition of the patient’s
alimentary canal. Make the provisional diagnosis:
87. 3 hours after a trauma, a young man developed bradycardia of 46/min., anisocoria D>S, hemi-
hyperreflexia S>D, hemihypesthesia on the left, and a convulsive disorder. The character of this
process needs to be clarified. What method of examination will be the most accurate for this
purpose?
Explanation
A cranial CT scan is a diagnostic tool used to create detailed pictures of features inside your head, such as your skull, brain, paranasal sinuses, ventricles, and eye sockets. CT stands for computed tomography, and this type of scan is also referred to as a CAT scan. The pictures created by a cranial CT scan are far more detailed than regular X-rays.
Electroencephalogram (EEG) is the most common test used to diagnose epilepsy, but in this case, the convulsive disorder is not the only abnormality we need to investigate. There are other disorders like bradycardia, anisocoria (greater on the right i.e. Dextra>Sinistra), hyperreflexia (more on the left i.e. Sinistra>Dextra) and hemihypesthesia. Hence, a brain CT scan is the best choice to start with in this case.
88. A 25-year-old woman complains of fatigue, dizziness, hemorrhagic rashes on the skin. She has
been presenting with these signs for a month. Blood test: erythrocytes - 1.0∙1012/L, Hb - 37 g/L,
color index - 1.1, leukocytes - 1.2∙109/L, platelets - 42∙109/L. What analysis would be the most
advisable for diagnosis-making in this case?
89. A 48-year-old woman has been hospitalized due to development of tachysystolic atrial fibrillation.
She has lost 5 kg of body weight within 2 months. On palpation there is a node in the left lobe of the
thyroid gland. What pathology resulted in the development of this condition?
90. Having studied the relationship between the distance from villages to the local outpatient clinics and
frequency of visits to the clinics among the rural population of this area, it was determined that the
rank correlation coefficient in this case equals -0.9. How can this relationship be characterized?
Explanation
The Spearman's Rank Correlation Coefficient is used to discover the strength of a link between two sets of data. This example looks at the strength of the link between the distance from villages to the local outpatient clinics and frequency of hospital visits.
Correlation is a bivariate analysis that measures the strength of association between two variables and the direction of the relationship. In terms of the strength of relationship, the value of the correlation coefficient varies between +1 and -1. A value of ± 1 indicates a perfect degree of association between the two variables. As the correlation coefficient value goes towards 0, the relationship between the two variables will be weaker. A correlation coefficient of zero indicates that no relationship exists between the variables. The direction of the relationship is indicated by the sign of the coefficient; a + sign indicates a positive relationship and a – sign indicates a negative relationship.
An inverse correlation, also known as negative correlation, is a contrary relationship between two variables such that when the value of one variable is high then the value of the other variable is probably low.
The value of the correlation coefficient ‘r’ can range from 0.0, indicating no relationship between the two variables, to positive or negative 1.0, indicating a strong linear relationship between the two variables.
|
Value of r
|
Indications
|
|
0.0
|
No linear relationship between the two variables
|
|
+1.0
|
Strong positive linear relationship; as X increases in value, Y increases in value also; or as X decreases in value, Y decreases also.
|
|
-1.0
|
Strong inverse linear relationship; as X increases in value, Y decreases in value; or as X decreases in value, Y increases in value.
|
Therefore, a value of -0.9 is very close to -1.0 and that will give us a strong inverse relationship.
91. A 63-year-old man complains of unmotivated weakness and pressing and bursting sensation in the
left subcostal area. According to him, these signs have been present for a year already. Previously
he was healthy. He took part in containment measures during the accident at the Chornobyl
Nuclear Power Plant. Objectively: the skin is pale, peripheral lymph nodes are not enlarged, the
liver is +3 cm, the spleen is +10 cm. Complete blood count: erythrocytes - 3.1∙1012/L, Hb - 100 g/L,
leukocytes - 46∙109/L, blasts - 2%, promyelocytes - 10%, myelocytes - 18%, band neutrophils -
27%, segmented neutrophils - 10%, lymphocytes - 12%, eosinophils - 6%, basocytes - 3%,
monocytes - 2%, erythrocyte sedimentation rate - 20 mm/hour. What is the most likely diagnosis?
92. At night a 2-year-old child with upper respiratory tract infection suddenly developed dyspnea with
labored inspiration. Objectively the skin is pale, perioral cyanosis and slight acrocyanosis are
observed. Breathing is loud, respiration rate is 32/min. Jugular, supra- and infraclavicular fossae
retract during breathing. Respiration is coarse on auscultation. Heart sounds are clear and
sonorous, heart rate is 120/min. What condition was complicated by the development of the upper
respiratory tract infection?
93. A 50-year-old patient was brought to a hospital with complaints of blood in urine. Urination is
painless and undisturbed. Macrohematuria had been observed for 3 days. Objectively: kidneys
cannot be palpated, suprapubic area is without alterations, external genitalia are non-pathologic.
On rectal investigation: prostate is not enlarged, painless, has normal structure. Cystoscopy
revealed no changes. What is the most likely diagnosis?
94. A 23-year-old woman came to the gynecological clinic. She complains of pain, itching, and burning
in her vulva, general weakness, indisposition, elevated body temperature up to 37.2°C, and
headache. On examination in the vulva there are multiple vesicles up to 2-3 mm in diameter with
clear contents against the background of hyperemia and mucosal edema. Make the provisional
diagnosis:
Explanation
Herpes simplex viruses are enveloped double stranded linear viruses. HSV-1 is also known as oral herpes (gingivostomatitis, keratoconjunctivitis etc) while HSV-2 is known as genital or neonatal herpes. The clinical presentation of genital herpes include pain, itching, dysuria, vaginal and urethral discharge, tender lymphadenopathy, appearance of herpes vesicles on the external genitalia, labia majora, labia minora, vaginal vestibule - for women; and glans penis, prepuce, shaft of the penis, and sometimes on the scrotum, thighs, and buttocks- for men.
Primary syphilis usually presents with a localized painless hard chancre on the genitals.
Cytomegalovirus is also known as human herpes virus-5, it is usually seen in immunocompromised patients and infected cells have characteristic ‘ owl's eye’ intranuclear inclusions.
95. After a pain attack in the right subcostal area, a 58-year-old woman with overnutrition developed
icteric skin and sclera, light-colored feces, and dark urine. Her abdomen is distended and painful on
palpation in the right subcostal area. Palpation detects liver enlargement by 2-3 cm. Blood test:
total bilirubin - 90 mcmol/L, conjugated bilirubin - 60 mcmol/L. What method of examination will be
the most informative for diagnosis clarification?
Explanation
From the question stem, it is evident that the patient has obstructive, mechanical or post-hepatic jaundice (icteric skin, light colored feces, dark urine).
Obstructive jaundice is a condition in which there is blockage of the flow of bile out of the liver. Therefore, it is caused by conditions that block the normal flow of bile from the liver into the intestines including: Biliary stricture (narrowing of the bile duct), cancer of the gallbladder or pancreas, Cholangitis (infection or inflammation of the common bile duct), Cholelithiasis (gallstones), Cysts of the bile duct, pancreatitis, parasitic infection, or trauma, including surgical complications.
ERCP (short for endoscopic retrograde cholangiopancreatography) is a procedure used to diagnose diseases of the gallbladder, biliary system, pancreas, and liver. During an ERCP, a gastroenterologist (doctor who specializes in treating diseases of the gastrointestinal system), uses a special endoscope (a long, flexible tube with a light and camera at the end) to examine the inside of the digestive system. The doctor identifies the place where the bile duct comes into the intestine and then feeds a tiny catheter (a plastic tube) into the duct and squirts in a contrast agent while X-rays are taken. The contrast agent allows the doctors to see the bile ducts, the gallbladder, and the pancreatic duct on the X-rays. Once the source of the problem is identified, the doctor may then treat it.
96. A 30-year-old woman made an appointment with the family doctor for scheduled vaccination of her
2-year-old child. What type of healthcare provides such medical services?
Explanation
According to levels of specialization, types of medical care include: Emergency, Primary, Secondary, Tertiary, palliative, medical rehabilitation and dentistry.
Primary medical care: involves care given by nurses, midwives, general physicians, family doctors, in polyclinics etc. Primary healthcare is the first contact a person has with the health system when they have a health problem.
Secondary medical care: When your primary care provider refers you to a specialist, you are then in secondary care. Secondary care simply means you will be taken care of by someone who has more specific expertise eg cardiologist, endocrinologist etc
Tertiary Medical Care: Once a patient is hospitalized and needs a higher level of specialty care within the hospital, he may be referred to tertiary care. Tertiary care requires highly specialized equipment and expertise. For example Cardiosurgery.
At this level, you will find procedures such as coronary artery bypass surgery, renal or hemodialysis, and some plastic surgeries or neurosurgeries.
97. A 38-year-old woman after physical overexertion suddenly developed palpitations, dyspnea, and a
dull pain in the cardiac area. For 10 years she has been registered for regular check-ups due to
rheumatism and mitral valve disease with non-disturbed blood circulation. Oblectively her pulse is
96/min., of unequal strength. Blood pressure is 110/70 mm Hg, heart rate is 120/min. ECG registers
small unevenly-sized waves in place of P-waves, R-R intervals are of unequal length. What is the
most likely diagnosis
98. A man was brought into the admission room after an overexposure to cold. He complains of sharp
pain in the small of his back and elevated body temperature up to 38°C. He took some aspirin.
Blood test: leukocytes - 10.5∙1012/L, eosinophils - 5%, band neutrophils - 8%, segmented
neutrophils - 51%, lymphocytes - 32%, monocytes - 4%, erythrocyte sedimentation rate - 28
mm/hour. Urinalysis: protein - 0.6 g/L, leukocytes - cover the whole vision field, large amount of
mucus. What is the most likely diagnosis?
99. After a surgery for a left thigh phlegmon the disease progression was complicated by sepsis. On
the 7th day after the surgery there are marked signs of a generalized inflammatory reaction, in
blood there are signs of toxic anemia and progressing hypoproteinemia, bilirubin levels are 40
mcmol/L, AST and ALT exceed the norm by 2.5 times. Oliguria persists (700 mL of urine per day).
Name the phase of sepsis progression
100. A 9-month-old infant presents with delayed tooth eruption and fontanel closure, weakness, and
excessive sweating. What type of hypovitaminosis is the most likely in this child?
101. A 24-year-old woman, a kindergarten teacher, has been sick for 2 days already. Disease onset was
acute. She presents with elevated body temperature up to 38.0°C, pain attacks in her lower left
abdomen, liquid stool in small amounts with blood and mucus admixtures 10 times a day. Pulse -
98/min., blood pressure - 110/70 mm Hg. Her tongue is moist and coated with white deposits. The
abdomen is soft, the sigmoid colon is painful and spastic. Make the provisional diagnosis:
Explanation
Bacterial gastroenteritis is caused by a variety of organisms, including Campylobacter, Salmonella, Shigella, Yersinia, Vibrio cholerae, Staphylococcus aureus, diarrheagenic Escherichia coli, Clostridium difficile, Clostridium perfringens, and non cholera Vibrio species. Shigellosis is also known as bacillary dysentery caused by the infection of the shiga toxin. It is characterised by High-fever, tenesmus, Profuse inflammatory, mucoid-bloody diarrhea and basically affects the large intestine. Commonly transmitted via fecal-oral route. This patient experiences pain in the sigmoid colon accompanied by profuse diarrhea (mixed with blood and mucus).
Salmonellosis presents often without blood and commonly transmitted with poultry products (eggs, omelette etc)
102. A 25-year-old woman was brought into the gynecological department with profuse bloody discharge
from her genital tracts. She is 12 weeks pregnant, the pregnancy is planned. Within the last 3 days
she was experiencing pains in her lower abdomen that eventually started resembling cramps, she
developed bleeding. Her skin is pale, pulse - 88/min., blood pressure - 100/60 mm Hg, body
temperature - 36.8°C. Vaginal examination: the uterus size corresponds with 11 weeks of
pregnancy, the cervical canal allows inserting 1 finger and contains fragments of the fertilized ovum,
the discharge is bloody and profuse. What is the most likely diagnosis?
Explanation
Abortion is the removal of pregnancy tissue, products of conception or the fetus and placenta (afterbirth) from the uterus. It is the extraction or the expulsion of the product of conception that weighs less than or equal to 500g. Abortions could either be spontaneous or Induced (legal or therapeutic abortion).
Spontaneous Abortion includes: threatened, inevitable, incomplete, complete, missed, or septic.
There are 3 classical features of Abortion: Bleeding per vagina, Abdominal pain and History of amenorrhea (physiological amenorrhea - the woman is pregnant, so no menses).
In this case, she is 12 weeks pregnant and the spontaneous abortion is in progress because the cervix is open (cervical canal allows 1 finger which means 2cm open). In threatened abortion, the cervix is closed.
103. A 23-year-old man complains of facial edemas, headache, dizziness, low urinary output, and urine
discoloration (dark red). These complaints arose after a case of acute tonsillitis. On examination
there are facial edemas, the skin is pale, temperature is 37.4°C; heart rate is 86/min., blood
pressure is 170/110 mm Hg. Heart sounds are muffled, the II heart sound is accentuated over the
aorta. What etiological factor is the most likely in this case?
104. A newborn with gestational age of 31 weeks presents with hypotonia and depressed
consciousness. Hematocrit is 35%, general cerebrospinal fluid analysis shows increased content of
erythrocytes and protein, and low glucose. These data correspond with the clinical presentation of:
105. A 37-year-old patient complains of pain in the spinal column, reduced mobility. The condition
persists for 7 years. ”Sway back” is observed, there is no movement in all spinal regions. X-ray
shows ”bamboo spine” vertebral column. What is the most likely diagnosis?
106. Human body receives from the atmosphere a number of chemicals. What type of action results in
the combined effect that is less than the sum of isolated effects of these chemicals on the body?
107. A 33-year-old man developed multiple rashes on the skin of his torso and extensor surfaces of his
upper and lower limbs. The rashes itch and occasionally fuse together and form plaques. The
elements of rash are covered with silver-white fine scales that easily flake off when scratched.
Grattage test results in three sequential phenomena: stearin spot, terminal film, and punctate
hemorrhage. What diagnosis can be suspected?
108. After eating shrimps, a 25-year-old man suddenly developed skin itching, some areas of his skin
became hyperemic or erupted into vesicles. Make the diagnosis:
109. A 58-year-old man complains of weakness and tumor-like formations that appeared on the anterior
surface of his neck and in the inguinal region. Palpation detects soft painless mobile cervical and
inguinal lymph nodes up to 2 cm in diameter. The liver protrudes by 2 cm from the edge of the
costal margin, the lower splenic pole is at the umbilical level. In blood: erythrocytes - 3.5∙1012/L, Hb
- 88 g/L, leukocytes - 86∙109/L, band neutrophils - 1%, segmented neutrophils - 10%, lymphocytes -
85%, eosinophils - 2%, basocytes - 0%, monocytes - 2%, erythrocyte sedimentation rate - 15
mm/hour, Gumprecht shadows. What is the most likely diagnosis?
110. A 28-year-old man complains of skin rash and itching on the both of his hands. The condition
persists for 1.5 years. The exacerbation of his condition he ascribes to the occupational contact
with formaldehyde resins. Objectively the lesion foci are symmetrically localized on both hands.
Against the background of erythema with blurred margins there are papulae, vesicles, erosions,
crusts, and scales. What is the most likely pathology?
111. A 73-year-old woman came to the family physician for one of her regular follow-up examinations.
Three months ago she was found to have type 2 diabetes mellitus. She was keeping to her diet and
exercise plan and taking phytopreparations. On examination her fasting glucose was within the
range of 7.8-8.6 mmol/L, HbA1c - 7.9%. Height - 164 cm, weight - 83 kg. What blood sugar-
controlling medicine should she be prescribed first in the course of her pharmacological therapy?
112. At night a 63-year-old woman suddenly developed an asphyxia attack. She has a 15- year-long
history of essential hypertension and had a myocardial infarction 2 years ago. Objectively her
position in bed is orthopneic, the skin is pale, the patient is covered with cold sweat, acrocyanosis
is observed. Pulse - 104/min. Blood pressure - 210/130 mm Hg, respiration rate - 38/min.
Pulmonary percussion sound is clear, with slight dullness in the lower segments; throughout the
lungs single dry crackles can be heard that become bubbling and non-resonant in the lower
segments. What is the most likely complication in this patient?
113. A 10-year-old boy, who was outdoors in windy and cold weather, developed moderate pain and
tingling in his fingers and toes. When he returned home, his parents noticed that the tips of his
fingers and toes were white and their sensitivity was lost. As the affected areas were warming up,
the fingers and toes developed tingling and painful sensations. Skin pallor changed into redness,
tingling stopped, mild itching and swelling of the fingers appeared. Determine the frostbite degree in
this child:
114. A 32-year-old woman complains of episodes of intense fear that occur without visible cause and
last for 10-20 minutes; the episodes are characterized by rapid pulse, sweating, labored breathing,
and vertigo. Specify the likely diagnosis:
115. A 7-year-old boy has been an inpatient for 1.5 months. He had been brought to the hospital with
complaints of edemas all over his body, low urine output, and headache. Clinical urinalysis: proteins
- 7.1 g/L, leukocytes - 1-2 in the vision field, erythrocytes - 3-4 in the vision field. During the course
of treatment the edemas gradually dissipated, headache abated, diuresis normalized. Daily urine
proteins - 3 g/L. Biochemical blood test: total protein - 43.2 g/L, urea - 5.2 mmol/L, cholesterol - 9.2
mmol/L. What glomerulonephritis syndrome is the most likely to be present in the patient?
116. A 62-year-old woman was brought into the admission room with complaints of severe burning
retrosternal pain and asphyxia. She has a 10-year-long history of essential hypertension.
Objectively her condition is moderately severe. She presents with skin pallor, cyanotic lips, and
vesicular respiration over her lungs. The H heart sound is accentuated over the aorta. Blood
pressure - 210/120 mm Hg, heart rate (pulse) - 76/min. ECG shows elevation of ST segment in the
leads I, AVL, and V5-V6. What is the most likely diagnosis?
117. A 35-year-old patient developed an epileptic attack with tonoclonic spasms that lasted for 3
minutes. After the attack the patient fell asleep but in 5 minutes the second attack occurred. The
first step of emergency aid would be to:
118. On the day 4 after the cesarean section a woman developed fever with body temperature up to
39°C and abdominal pain. Pulse - 104/min. She vomited twice. The patient is sluggish, her tongue
is dry and has gray coating. The abdomen is distended. Signs of peritoneal irritation are positive in
all segments. Peristalsis cannot be auscultated. No passage of gas occurs. Uterine fundus is
located at the level of the navel. The uterus is painful on palpation. The discharge is moderate and
contains blood and pus. What is the most likely diagnosis?
119. On the 15th day after a small trauma of the right foot, the patient developed indisposition,
fatigability, irritability, headache, elevated body temperature, and sensation of constriction, tension,
and twitching in the muscles of the right shin. What disease can be suspected?
120. A 57-year-old patient complains of dyspnea at rest. The patient presents with orthopnea,
acrocyanosis, bulging cervical veins. On percussion: dull sound over the lower lung segments. On
auscultation: no respiratory sounds. Heart rate is 92/min. Right-sided cardiac dilatation is observed.
The liver is +7 cm. Shins are swollen. Pleural effusion is suspected. What indicator would confirm
the presence of transudate in this case?
121. A 38-year-old woman works in flax processing, she dries flax. She came to the hospital complaining
of difficult breathing, constricting sensation in her chest, and cough attacks. These signs appear on
the first day of her working week and gradually diminish on the following days. What respiratory
disease is likely in this case?
122. A 30-year-old man came to the family physician. 2 months ago he underwent a surgery for open
fracture of the humerus. On examination the patient’s condition is satisfactory; in the area of the
postoperative wound there is a fistula that discharges a small amount of pus; the area itself is red;
fluctuation is detected. X-ray shows destruction of the humerus with sequestra. What complication
did the patient develop during the postoperative period?
123. A 35-year-old man suffers from insulin-dependent diabetes mellitus and chronic cholecystitis. He
takes NPH insulin: 20 units in the morning and 12 units in the evening. After a meal he developed
pain in the right subcostal area, nausea, vomiting, sleepiness, and increased polyuria. What
prehospital measures will be the most effective for prevention of crisis within the next several
hours?
124. A 38-year-old woman complains of weakness, sleepiness, pain in the joints, weight gain despite
low appetite, and constipations. She presents with dry and thickened skin, puffy and amimic face,
narrowed palpebral fissures, thick tongue, and deep hoarse voice. Her heart sounds are weak,
pulse is 56/min. Low levels of free T4 are observed. This patient needs to take the following on a
regular basis:
125. A 40-year-old man claims that his wife is cheating on him and presents a ”proof” of her infidelity. He
repeatedly initiated scandals with his wife at home and at work, demanding that she confess her
infidelity, insulted her, and threatened to kill her. What preventive measures should be taken against
socially dangerous actions on his part?
126. Having examined a 52-year-old patient, the doctor diagnosed him with obesity (body mass index -
34 kg/m2, waist circumference - 112 cm) and arterial hypertension (170/105 mm Hg). 2-hour
postprandial blood sugar is 10.8 mmol/L. What biochemical blood analysis needs to be conducted
to diagnose the patient with metabolic syndrome X?
Explanation
Metabolic syndrome X is a group of risk factors which includes high blood pressure, high blood sugar, high triglycerides, low HDL cholesterol, and belly fat - that increases risk of heart disease and diabetes. Diet, exercise, and medications can help improve this condition.
From the question stem, the 52 year old patient has arterial hypertension (170/105mmHg); High blood sugar (10.8mmol/L 2hrs post prandial); Belly fat (112cm Waist circumference, BMI - 34 kg/m obesity). At this point, we are only left with the lipid profile which will tell us the triglyceride level, LDL, and HDL cholesterol levels. 127. A 10-year-old boy was brought into the hospital with complaints of expiratory dyspnea, respirations
are 30/min. He explains his state by a change in the weather conditions. For the last 4 years the
boy has been registered for regular check-ups due to his diagnosis of third degree persistent
bronchial asthma. To provide emergency aid for this child, first he needs to be given:
128. A 43-year-old man complains of a protrusion in the right inguinal region, that enlarges due to strain.
He has been presenting with this condition for 6 months. Within this period the protrusion has
grown. Objectively in the right inguinal region an elastic protrusion 8x5 cm is visible. On palpation it
disappears, leaving an empty space 4x4 cm between the pedicles of the Poupart ligament. ”Cough
push” sign is positive over this opening. Make the diagnosis:
Explanation
Hernia occurs when an organ pushes through an opening in the muscle or tissue that holds it in place. For example, the intestines may break through a weakened area in the abdominal wall.
The most common symptom of a hernia is a bulge or lump in the affected area. For example, in the case of an inguinal hernia, you may notice a lump on either side of your pubic bone where your groin and thigh meet. You may find that the lump disappears when you’re lying down. You’re more likely to feel your hernia through touch when you’re standing up, bending down, or coughing (positive cough push sign). Discomfort or pain in the area around the lump may also be present.
In the question stem, the mass was noticeable between the Poupart’s ligament which is another name for inguinal, or groin ligament. Inguinal hernias are the most common type of hernia. These occur when the intestines push through a weak spot or tear in the lower abdominal wall, often in the inguinal canal. This type is also more common in men.
These hernias are more common in men because the testicles descend through the inguinal canal shortly after birth. The canal is supposed to close almost completely behind them. Sometimes the canal doesn’t close properly, leaving a weakened area.
Inguinal Hernia can be reducible or irreducible. Reducible hernia: is one which can be pushed back into the abdomen by putting manual pressure to it. Irreducible/Incarcerated/Strangulated hernia: is one which cannot be pushed back into the abdomen by applying manual pressure.
Lymphadenitis is associated with inflamed and painful inguinal lymph nodes. Femoral hernia will be noticed in the femoral triangle way below the inguinal canal. Cyst of the spermatic cord is not reducible and it will be located in the testis.
The arcuate line of rectus sheath, linea semicircularis, arcuate line, or Douglas' line is a horizontal line that demarcates the lower limit of the posterior layer of the rectus sheath. It is also where the inferior epigastric vessels perforate the rectus abdominis. Hernia can be located here as well. But this is more of a midline and below the umbilicus hernia location and not related to the inguinal canal or inguinal/poupart ligament.
129. A 39-year-old man, a battery attendant, suddenly developed weakness, loss of appetite,
nonlocalized colicky abdominal pains, and nausea. Objectively his skin is gray; there is a pink-gray
stripe on his gums; the stomach is soft and sharply painful. Blood test detected erythrocytes with
basophilic stippling and anemia. The patient has a history of peptic ulcer disease of the stomach.
Constipation tends to occur every 3-4 days. What is the most likely provisional diagnosis?
Explanation
Lead-based paint and its dust, usually found in older buildings, are common sources of exposure. Young children are especially at risk. Adults - occupational exposure (welding, batteries, ammunition).
Symptoms include developmental delays, abdominal pain, constipation, headaches, irritability, memory problems, inability to have children, and tingling in the hands and feet.. At very high levels, it can be fatal.
Lead in the body is distributed to the brain, liver, kidney and bones. It is stored in the teeth (pink-gray stripe on the patient’s gum) and bones, where it accumulates over time.
Ferrochelatase and Delta-aminolevulinic acid dehydratase are enzymes necessary for the synthesis of heme. In lead poisoning, these enzymes are inhibited leading to anemia and an increased delta aminolevulinic acid content in urine. This presents with microcytic anemia (basophilic stippling in peripheral smear, ringed sideroblast in bone marrow), GI and kidney disease. The above patient presents with signs of asthenic vegetative syndrome coupled with the above stated reasons confirming a case of lead poisoning.
130. A newborn has Apgar score of 9. When should this infant be put to the breast?
131. In the process of hiring, a prospective employee has undergone preventive medical examination
and was declared fit to work in this manufacturing environment. What type of preventive medical
examination was it?
132. A 45-year-old man underwent a cardiac surgery one week ago. His general state has been
deteriorating since then: dyspnea at rest, retrosternal pain that irradiates to the neck, marked
weakness. Objectively his body temperature is hectic. His cardiac borders are expanded, apical
beat is weakened. Auscultation detects pericardial friction rub. What is the most likely diagnosis?
Explanation
A pericardial friction rub, also pericardial rub, is an audible medical sign used in the diagnosis of pericarditis. A pericardial friction rub is highly specific for acute pericarditis. It is generally heard over the left sternal border, louder at inspiration and on bending forward.
The pericardium is a thin, two-layered, fluid-filled sac that covers the outer surface of the heart. It provides lubrication for the heart, shields the heart from infection and malignancy, and contains the heart in the chest wall. It also keeps the heart from over-expanding when blood volume increases, which keeps the heart functioning efficiently.
Acute pericarditis is an inflammation of the pericardium characterized by pericarditic chest pain, pericardial friction rub, and serial electrocardiographic (ECG) changes (eg, new widespread ST-elevation or PR depression; new/worsening pericardial effusion).
There are many causes of pericarditis: viral, fungi, bacterial, parasitic, autoimmune. Your risk of pericarditis is higher after a heart attack, heart surgery (postpericardiotomy syndrome), radiation therapy or a percutaneous treatment, such as cardiac catheterization or radiofrequency ablation. Just as the patient in question underwent a cardiac surgery one week ago.
133. A 48-year-old woman complains of disturbed menstrual cycle: her periods last for 7-9 days and are
excessively profuse throughout the last half-year. She notes occasional hot flashes in her head,
insomnia, irritability, and headaches. Her skin is of normal color. Blood pressure - 150/90 mm Hg,
pulse - 90/min., rhythmic. The abdomen is soft and painless. Bimanual examination shows no
uterine enlargement, the appendages cannot be detected. The vaginal fornices are free. What is
the most likely diagnosis?
Explanation
When a woman reaches her 40s or 50s she begins to experience a natural decline in reproductive hormones, which eventually leads to Menopause. Menopause is signalled by 12 months since last menstruation. However, the period - perimenopausal, i.e. premenopause and immediate post menopause when the female reproductive functions begins to decline is called Climacteric period.
Peri- and postmenopausal women often seek medical help, and climacteric symptoms are their most common reason for doing so. These symptoms are due to changes in ovarian function during the menopause. The transition from full ovarian function in the premenopausal period to a complete lack of ovarian estrogen synthesis in the postmenopausal period is, fundamentally, a normal aspect of human physiology.
Climacteric, is that particular phase in ageing women, which marks the transition from the reproductive phase to non-reproductive state and is often associated with symptomatology, referred to as climacteric syndrome.
Symptoms: vasomotor symptoms (hot flashes, diaphoresis); vaginal dryness; sleep disturbances; mood changes; urinary tract symptoms; sexual problems (loss of libido, dyspareunia, other) etc.
NB: just as menarche doesn't start with regular periods, so is menopause. Before a full blown menopause, women will begin to have irregular and abnormal periods then it ceases completely. That’s why the patient in question still saw her period (but it's disturbed menstrual cycle - meaning it's not regular).
134. A 62-year-old patient has been hospitalized with complaints of pain in the thorax on the right during
breathing, dyspnea, and dry cough. Ten days ago he slipped and fell hitting his right side. On
examintaion: the patient lies on the left side. The right side of the thorax lags during breathing. On
the right there are crepitation and pain in the III-IV ribs. Dullness of percussion sound and sharply
diminished breath sounds can be observed. On X-ray: signs of exudate, fracture of the III- IV ribs.
On pleurocentesis: blood is detected. Choose the further tactics:
135. A 19-year-old young man complains of cough with expectoration of purulent sputum in the amount
of 100 mL per day, hemoptysis, dyspnea, increased body temperature up to 37.8°C, general
weakness, weight loss. The patient’s condition lasts for 4 years. Exacerbations occur 2-3 times a
year. The patient presents with malnutrition, pale skin, cyanosis of the lips, drumstick (clubbed)
fingers. Tympanic percussion sound in the lungs, weakened respiration, numerous various moist
crackles in the lower pulmonary segments on the left can be observed. In blood: erythrocytes -
3.2∙1012/L, leukocytes - 8.4∙109/L, ESR - 56 mm/hour. On X-ray: lung fields are emphysematous,
the left pulmonary root is deformed and dilated. What is the most likely diagnosis?
136. A 72-year-old man with pneumonia complains of marked dyspnea, chest pain, severe cough with
expectoration, t° is 39.5-40°C, no urination for a whole day. Objectively the patient is conscious.
Respiratory rate is 36/min. Over the right lower pulmonary lobe percussion sound is dull; on
auscultation there is bronchial respiration and numerous moist crackles. Blood pressure is 80/60
mm Hg. Heart rate is 120/min. Heart sounds are muffled, there is tachycardia. What tactics should
the family doctor choose in the management of this patient?
137. 2 hours after eating unknown mushrooms, a 28-year-old man sensed a decrease in his mobility and
deterioration of his ability to focus. This condition was then followed by a state of agitation add
agression. On examiantion he is disoriented and his speech is illegible. 4 hours later he developed
fetor hepaticus and lost his consciousness. What syndrome can be observed in this patient?
Explanation
Amanita phalloides is the most common and fatal cause of mushroom poisoning. This mushroom contains amanitins, which are powerful hepatotoxins that inhibit RNA polymerase II in the liver. Amanita phalloides intoxication has four consecutive phases in the classical course: lag phase, gastrointestinal phase, apparent convalescence, and acute liver failure. Acute Liver Failure is the last phase in which the transaminases rise dramatically and liver and renal function deteriorate. This process results in hyperbilirubinemia, coagulopathy, hypoglycemia, acidosis, hepatic encephalopathy, and hepatorenal syndrome.
Fetor hepaticus is associated with severe liver disease, which causes scarring and poor functioning of your liver.
138. A 20-year-old man was hospitalized on the 9th day of the disease. He attributes his disease to
eating of insufficiently thermally processed pork. At its onset this condition manifested as periorbital
edemas and fever. Objectively his body temperature is 38.5°C. The face is puffy and the eyelids
are. markedly swollen. Palpation of gastrocnemius muscles is sharply painful. Blood test shows
hypereosinophilia. What is the etiology of this disease?
Explanation
Trichinellosis, also called trichinosis is caused by the roundworm (nematode) - Trichinella spiralis. Transmission: undercooked meat especially pork.
When humans eat undercooked meat containing trichinella larvae, the larvae mature into adult worms in the small intestine over several weeks. The adult worms then produce larvae that travel through various tissues, including muscle.
About a week after infection, the adult female worms produce larvae that go through the intestinal wall, enter your bloodstream, and eventually burrow into muscle or other tissue. This tissue invasion can cause:
-
High fever
-
Muscle pain and tenderness
-
Swelling of the eyelids or face (periorbital edema)
-
Weakness
-
Headache
-
Sensitivity to light
-
Pink eye (conjunctivitis)
Treatment: Bendazoles
Echinococcus: etiology - Echinococcus granulosus; Disease - hydatid cysts (eggshell calcification) in liver; Transmission - ingestion of eggs in food contaminated with dog feces. Sheep are an intermediate host.
Leptospira: etiology - Leptospira interrogans; spirochete with hook-shaped ends found in water contaminated with animal urine. Disease - flu-like symptoms, myalgias, jaundice, photophobia
Ascarididae: etiology - Ascaris lumbricoides (giant roundworm); Disease - may cause obstruction at ileocecal valve, biliary obstruction, intestinal perforation. Transmission - fecal-oral
Trichuris: etiology - Trichuris trichiura (whipworm); Disease - often asymptomatic, loose stool, anemia, rectal prolapse in children. Transmission - fecal-oral
139. A 1.5-month-old child on breasfeeding presents from birth with daily vomiting, irregular liquid foamy
feces, and meteorism, which are resistant to antibacterial and probiotic therapy; no increase of
body mass is observed. The child’s condition improved, when breastmilk was substituted with ”NAN
low lactose” formula. What pathology is it?
140. A 45-year-old woman complains of intolerable paroxysmal facial pain on the left with attacks that
last for 1-2 minutes. Attacks are provoked by chewing. The disease onset was two months ago
after the overexposure to cold. Objectively: pain at the exit points of the trigeminal nerve on the left.
Touching near the wing of the nose on the left induces a pain attack with tonic spasm of the facial
muscles. What is the most likely diagnosis?
141. It is the 3rd day after the first normal term labor; the infant is rooming-in with the mother and is on
breastfeeding. Objectively: the mother’s general condition is satisfactory. Temperature is 36.4°C,
heart rate is 80/min., BP is 120/80 mm Hg. Mammary glands are soft and painless; lactation is
moderate, unrestricted milk flow. The uterus is dense, the uterine fundus is located 3 finger widths
below the navel. Lochia are sanguino-serous, moderate in volume. Assess the dynamics of uterine
involution:
142. A 24-year-old pregnant woman on her 37th week of pregnancy has been brought to the maternity
obstetric service with complaints of weak fetal movements. Fetal heartbeats are 95/min. On vaginal
examination the uterine cervix is tilted backwards, 2 cm long, external orifice allows inserting a
fingertip. Biophysical profile of the fetus equals 4 points. What tactics of pregnancy management
should be chosen?
143. 2 hours after a traffic accident a 28-year- old man in a grave condition was brought to a hospital.
The patient complains of abdominal pain. He received a blow to the abdomen with the steering
wheel. Objective examination revealed the following: the abdomen does not participate in
respiration, is tense and acutely painful on palpation; the abdominal muscles are defensively tense,
peritoneal irritation signs are positive, hepatic dullness is absent. BP is 90/60 mm Hg, heart rate is
120/min. What further treatment tactics should be chosen?
144. A 13-year-old girl for the last two weeks has been complaining of dyspnea and shin and foot
edemas that appear after a physical exertion. In the morning the edemas significantly decrease.
Clinical examination revealed enlarged liver and coarse systolic murmur over the heart area. Blood
test and urinalysis are without changes. What is the most likely cause of edemas in this child?
145. A patient has the second and third degree burns of the 15% of the body surface. On the 20th day
after the trauma the patient presents with sharp increase of body temperature, general weakness,
rapid vesicular respiration; facial features are sharpened, BP is 90/50 mm Hg, heart rate is 112/min.
What complication is it?
146. In the factory cafeteria there was an outbreak of food poisoning. Clinical presentation indicates
staphylococcal etiology of this disease. 15 people are sick. To confirm the diagnosis of food
poisoning, samples need to be sent to the laboratory. What samples should be obtained for
analysis?
147. A 3-year-old child has been brought to a hospital with complaints of pain in the legs, fever, and loss
of appetite. Objectively: pale skin and mucosa, hemorrhagic rash. Lymph nodes are enlarged,
painless, dense and elastic, not matted together. Bones, joints, and abdomen are painful. The liver
and spleen are enlarged. Hemogram: Hb - 88 g/L, color index - 1.3, platelets - 80∙109/L, leukocytes
- 25.8∙109/L, lymphoblasts - 70%, ESR - 52 mm/hour. Make the provisional diagnosis:
148. A 46-year-old woman has diarrhea with abdominal distension, loss of body mass, and large
amounts of porridge-like foul-smelling stool without blood streaks or tenesmus. Objective
examination detects moderate tenderness in the mesogastrium and left abdominal flank. Feces
analysis detects steatorrhea with neutral fat and creatorrhea. What prescription would be the most
advisable in this case?
Explanation
The pancreas plays a major role in digestion (its exocrine function). It produces digestive enzymes such as; trypsin and chymotrypsinogen (for protein digestion), Amylase (for carbohydrate digestion), lipase ( for breakdown of fats).
Recall that the pancreas has both endocrine and exocrine functions; for the exocrine part, it produces enzymes that aid in digestion such as amylase, lipase, trypsin. Absence of these enzymes will lead to symptoms such as steatorrhea (fats in feces), creatorrhea (undigested muscles in feces) etc.
In pathologies relating to the pancreas such as pancreatitis, this function is affected leading to indigestion and absorption issues. For example, due to a disruption in the release of lipase, fat breakdown is negatively affected leading to malabsorption and its appearance in stool (steatorrhea). Likewise a disruption in chymotrypsin and trypsin secretion will lead to an abnormal excretion of muscle fibres in faeces (creatorrhea).
Therefore, the best prescription to remedy the situation is to prescribe a multi-enzyme preparation - Trypsin; Chymotrypsin; Amylase; Lipase.
149. A 7-year-old girl has been twice treated with antibacterial agents for urinary tract infection. US
shows no severe renal defects. The child presents with recurrence of leukocyturia and bacteriuria,
elevated body temperature up to 38.5°C, and pain in her left lumbar area. What examination should
be conducted first to clarify the cause of urinary infection recurrence?
Explanation
A micturating cystourethrogram (MCUG) is a scan that shows how well your child’s bladder works. It is used to diagnose why your child may have urinary tract infections. It is also used to show up any abnormalities with your child’s urinary system.
Various types of scan such as CT, ultrasound and x-rays (most other options listed) can show the size and shape of your child’s bladder, but not how it is emptying.
A micturating cystourethrogram or voiding cystourethrography is a procedure allowing the urethra to be x-rayed using contrast dye passing from the bladder through the urethra. It is a frequently performed technique for visualizing a person's urethra and urinary bladder while the person urinates. The bladder is first filled with x-ray contrast dye by inserting a urinary catheter into the bladder through the urethra. A contrast medium is a clear liquid that shows up on an X-ray. Babies and young children will naturally pee when the bladder is full. Older children will be given a jug to pee into while lying on the table, when they feel ready. The radiographer will take a few X-ray pictures while your child is peeing, which you will be able to see on the screen.
For this patient having recurrent Urinary Tract Infections, it could be as a result of vesicoureteral reflux. This method is commonly used in the diagnosis of vesicoureteral reflux.
Recall that the US shows no severe renal defects, so there is no urgent need to repeat retrograde pyelography, excretory urography and radioisotope renography. Intravenous urography (IVU), also referred to as intravenous pyelography (IVP) or excretory urography (EU), is a radiographic study of the renal parenchyma, pelvicalyceal system, ureters and the urinary bladder.
Since the question states that there is no renal defect, we are more concerned about the lower urinary tract which makes micturating cystourethrography the best choice.
150. A 30-year-old man was brought to the neurosurgical department with complaints of constant
headaches, nausea, vomiting, fever, and weakness of the right-side limbs. Anamnesis states that
one month ago the patient had a surgery for left-sided suppurative otitis and mastoiditis. He has
been undergoing treatment in an ENT department. Approximately 2 weeks ago the temperature
increased, and the patient developed headaches. Objectively: heart rate - 98/min., BP - 140/90 mm
Hg, temperature - 38.3°C. Neurologically manifested stiff neck: bilateral Kernig’s symptom,
unsteadiness during the Romberg’s maneuver. Computer tomography of the brain revealed a three-
dimensional growth with a capsule in the left hemisphere. Make the diagnosis:
151. A 35-year-old pregnant woman with degree 1 essential hypertension, developed edemas and
headache at the 33 week of her pregnancy. Objectively her general condition is satisfactory, blood
pressure - 160/100 mm Hg, normal uterine tone. Fetal heart rate is 140/min., rhythmic. She was
diagnosed with daily proteinuria - 4 g/L, daily diuresis - 1100 mL. Creatinine - 80 mcmol/L, urea - 7
mmol/L, platelets - 100∙109/L. What complication of pregnancy occurred?
Explanation
Preeclampsia, a pregnancy-specific condition in which hypertension develops after 20 weeks of gestation in a previously normotensive woman. It is characterized by hemoconcentration, hypertension, and proteinuria. The following are the differences between a mild and severe Preeclampsia:
However, some texts also classify Moderate Pre-eclampsia on the following criteria:
Diastolic Blood Pressure: 100 - 109mmHg
Proteinuria: 0.3 - 5.0 g in 24hrs
Others: Edema (face and/or hands).
|
MIld Preeclampsia
|
Severe Preeclampsia
|
|
BP reading of 140/90 mm Hg twice, 4-6 hr apart
Proteinuria of 0.3 g/L in a 24 hr specimen or >0.1 g/L in a random day-time specimen on two or more occasions 6 hr apart
Dependent edema, some puffiness of eyes, face, fingers; pulmonary edema absent
Output matching intake, ≥30 ml/hr or <650 ml/24 hr
|
Rise to >160/110 mm Hg on two separate occasions 4-6 hr apart with pregnant woman on bed rest
Proteinuria of >0.5 g/L in 24 hr
Generalized edema, noticeable puffiness; eyes, face, fingers; pulmonary edema possibly present
<20 ml/hr or <400 ml to 500 ml/24 hr
|
152. A 1-year-old child with a case of URTI suddenly developed noisy respirations with difficult
inspiration, intercostal retractions, and barking cough on the 2nd night after the disease onset.
What is the most likely diagnosis?
153. During regular preventive gynecological examination a 30-year-old woman was detected to have
dark blue punctulated ”perforations” on the vaginal portion of the uterine cervix. The doctor
suspects endometriosis of the vaginal portion of the uterine cervix. What investigation method
would be most informative for diagnosis confirmation?
154. The burns unit received a patient, who 6 hours ago during a fire received flame burns. On the
patient’s body there is gray-brown area of necrosis that covers 3/4 of the body perimeter.
Occasionally there are small blisters with hemorrhagic contents and patches of shredded
epidermis. What local therapy is necessary in this case?
155. A 40-year-old man, a welder, uses manganese electrodes in his line of work (18 years of
experience). He complains of difficulties with writing, bad mood, inertness, gait abnormalities,
problems with speech, and hand tremors. Objectively the following is observed in the patient:
hypomimia, increased muscle tone of plastic type, and quiet monotonous speech, tremor of the
tongue, pill-rolling tremor of the fingers, and retropulsion. What syndrome developed in this patient
due to manganese poisoning?
156. A young man has made an appointment with the dermatologist. He complains of a painful facial
rash in the beard and mustache area. This condition has been persisting for several weaks already.
After shaving, the patient’s condition aggravates. The diagnosis of sycosis is made. What primary
morphological elements can be observed in the rash in this case?
Explanation
Sycosis is a chronic inflammatory disease involving the hair follicles, especially the bearded part of the face and marked by papules, pustules, and tubercles perforated by hairs with crusting.
Primary morphological elements include - Macule, Papule, Pustule, Patch, Vesicle etc.
Papules are elevated solid skin lesion <1cm. Pustule - vesicle containing pus.
157. A 22-year-old postparturient woman on the 12th day after the normal childbirth informs of elevated
body temperature up to 39°C for the last 3 days and pain in her right mammary gland. The right
mammary gland is enlarged, hot to touch, tense, hyperemic, and painful. Palpation reveals there a
dense infiltration 8x8 cm with a fluctuation in its center. What is the most likely diagnosis?
158. During analysis of morbidity in the city, it was determined that age structure of population is different
in each district. What statistical method allows to exclude this factor, so that it would not skew the
morbidity data?
159. A boy had a foreign body removed from under his nail plate. 3 days later he developed a sharp
throbbing pain at the end of his distal phalanx, which intensifies when the phalanx is pressed,
hyperemia of the nail fold, elevated body temperature up to 38.5°C, and nail plate discoloration.
Make the diagnosis:
Explanation
Panaritium or Whitlow - an acute purulent inflammation of tissues of the finger or feet.
Different types include; A. Surface shape - paronychia, subungual, cutaneous, subcutaneous, B. Deep shape - bone, joint, tendon, pandactylitis.
Subungual whitlow - characterized by an accumulation of pus under the nail plate. With advanced processes seen under one of its edges.
Articular whitlow - occurs more frequently after finger injury to the back surface of the joint. The pain is intense, skin furrows in the joint are smoothed, the skin is red, because of the swelling of the finger becomes fusiform. Trying to bend the finger leads to a sharp increase in pain. In advanced cases, the joint is destroyed. There is an unnatural mobility, crunching sensation in the area of diseased joints.
Bone whitlow - develops during the transition inflammation of soft tissue or bone by direct injury (injection sewing needle, chips, fish bone). In case the inflammation of the soft tissues surrounding the bone, after a period of apparent improvement complete recovery does not occur. The pain is constant aching in nature, formatted fistula with purulent discharge meager. Finger gradually thickens, its functions are completely lost.
Tendon whitlow - a purulent process in subcutaneous felons without proper treatment can spread to the flexor tendons of fingers. It comes with significant deterioration. Throbbing, pulling pain spreads throughout the fingers. All fingers along the length present with edema, red. Interphalangeal creases smoothed. Finger becomes like a sausage and slightly bent. This forced position reduces tendon tension and reduces pain.
Pandactylitis - purulent inflammation of all tissues of the finger, accompanied by headache, high body temperature. Pandactylitis may develop as a result of injury to the finger, but more likely it is untreated simple felons. 160. A woman with atopic bronchial asthma was found to have one allergen to dog hair +++. Carpets
were removed from the apartment, the apartment was renovated, and air conditioner was installed.
However, recurrent asphyxia attacks still occur every night, despite the patient undergoing
pathogenetic therapy. What long-term treatment tactics can help this patient to decrease her
sensitivity to the allergen?
161. A 38-year-old woman developed a medical condition 7 days after her return from Bangladesh.
Periodical elevation of temperature was accompanied by chills and excessive sweating. She was
diagnosed with tropical malaria. Next day her condition further deteriorated: body temperature -
38°C, inertness, periodical loss of consciousness, generalized seizures, tachycardia, hypotension,
and icteric skin. What complication can be suspected in this case?
Explanation
Poorly treated malaria often leads to the development of cerebral malaria. Cerebral malaria is the most severe neurological complication of infection with Plasmodium falciparum malaria. It is a clinical syndrome characterized by coma and asexual forms of the parasite on peripheral blood smears.
The World Health Organization defines cerebral malaria as a clinical syndrome characterized by coma at least 1 hour after termination of a seizure or correction of hypoglycemia, asexual forms of Plasmodium falciparum parasites on peripheral blood smears and no other cause to explain the coma.
Patients develop fever, headache, body ache, loss of consciousness, seizures and, progressively delirium, then coma. Anemia, hemoglobinuria, jaundice, shock, renal failure, lactic acidosis, abnormal bleeding, pulmonary edema, and adult respiratory distress syndrome may also develop. Some develop cortical infarcts and cerebral venous or dural sinus thrombosis as part of a disordered coagulation.
162. On laboratory investigation of a pork sample there is 1 dead trichinella detected in 24 sections. This
meat should be:
163. A 43-year-old man, a coal-face worker with 15-year-long record of work, complains of cough,
thoracic pain, and dyspnea. The cough is mild, usually dry, occurs mostly in the morning. The pain
is localized in the interscapular region and aggravates during a deep intake of breath. Dyspnea
occurs during physical exertion. Vesicular respiration in the lungs is weakened. Heart sounds are
rhythmic, hieart rate is 86/min., blood pressure is 135/80 mm Hg. The abdomen is soft and
painless. X- ray shows micronodular pulmonary fibrosis. Make the provisional diagnosis:
Explanation
The patient in question is a coal-face worker for 15 years.
Pneumoconiosis are professional diseases caused by long inhalation of an industrial dust and described by chronic diffuse aseptic inflammation of lungs with development of pneumofibrosis.
Carboconiosis includes anthracosis, grafitosis, carbon black pneumoconiosis. It is pneumoconiosis from coal dust exposure with varying degrees of coalification, which is the main criterion of its fibrogenic properties.
Berylliosis: exposure to beryllium and its compounds and It is associated with aerospace manufacturing, microwave semiconductor electronics, beryllium mining or manufacturing of fluorescent light bulbs.
Byssinosis is caused by inhaling hemp, flax, and cotton particles and is sometimes referred to as brown lung disease. It’s a form of occupational asthma.
Siderosis: excess iron in the body. Also known as pulmonary siderosis or Welder's disease. Commonly seen with welding, grinding, foundry work, paint manufacture or iron ore mining.
Hard-metal pneumoconiosis is caused by the inhalation of fine particles of hard metals, such as cobalt, tungsten, nickel, and titanium. Metal workers and persons who sharpen tools or polish diamonds are at increased risk of the condition.
164. A district doctor has diagnosed one of his patients with dysentery. What accounting document
reflects this type of morbidity?
165. A patient has gradually lost consciousness. The skin is pale and dry. There is a smell of ammonia
from the mouth. Respirations are deep and noisy. Heart sounds are muffled, pericardial friction rub
is present. Blood pressure is 180/130 mm Hg. Blood test: Hb - 80 g/L, leukocytes - 12∙109/L, blood
glucose - 6.4 mmol/L, urea - 50 mmol/L, creatinine - 1200 mcmol/L, blood osmolarity - 350
mOsmol/L. No urinary excretion. Make the diagnosis:
166. Clinical statistical investigation was performed to determine effectiveness of a new pharmacological
preparation for patients with ischemic heart disease. What parametric test (coefficient) can be used
to estimate the reliability of the results?
167. A woman in her early- to mid-thirties has lost her consciousness 3-5 minutes ago. On examination:
the skin is pale, no pulse over the carotid arteries, no spontaneous respiration, pupils are dilated;
the patient is nonresponsive, presents with atony. The patient’s condition can be determined as:
Explanation
Preagony, terminal pause, Agony, clinical and biological death all refer to terminal states of the body.
heart sounds are weak, pulse is thready, systolic blood pressure is
lower than the critical level of 70 mm Hg; external respiration is
weak and not effective, tidal volume and respiratory frequency are
inadequate; functions of parenchymal organs are violated. Preagony
can last for minutes, hours or even days.
-
Terminal pause- patient faints, blood pressure and pulse become hard to measure, respiratory arrest appears and reflexes are lost. Lasts for minutes.
-
Agony- Muscular tone, reflexes and external respiration (chaotic, with auxiliary respiratory muscles participation) are restored.
-
Clinical death- absence of pulse, dilated pupil and lack of photoreaction, gray or cyanotic skin colour (skin is pale), unconsciousness, lack of reflexes and muscular atony. No spontaneous respiration.
-
Biological death- Irreversible changes in the body especially the CNS.
168. A 35-year-old woman complains of high body temperature and pain in the upper outer quadrant of
her right buttock, which developed after an injection. She has been presenting with this condition
for 3 days. At the site of injection the skin is hyperemic; there is a painful infiltrate with an area of
softening in its center. The woman is diagnosed with a postinjection abscess of the right buttock.
What tactics should the surgeon choose in this case?
Explanation
Intramuscular injections can lead to local infectious complications, such as abscesses, skin necrosis, or intra-articular infections. Abscess formation following intramuscular injections is rare and they are most commonly seen in immunocompromised individuals.
An abscess is a confined collection of pus surrounded by inflamed tissue. Most abscesses are found on the extremities, buttocks, breast, axilla, groin, and areas prone to friction or minor trauma, but they may be found in any area of the body. Abscesses are formed when the skin is invaded by microorganisms.
Treatment of an abscess is primarily through incision and drainage (I&D). Smaller abscesses (<5 mm) may resolve spontaneously with the application of warm compresses and antibiotic therapy. Larger abscesses will require I&D as a result of an increase in collection of pus, inflammation, and formation of the abscess cavity, which lessens the success of conservative measures.
169. A woman has been working as a polisher for a year and a half. Her workstation is equipped with a
grinding machine (grinding wheels). She complains of white discoloration of her fingers and toes
that appears when she is nervous. Objectively there are no changes in the coloration of the distal
segments of her limbs. Grip strength measured with a dynamometer is 25 kg, algesimetry findings
are 0.1; 0.3; 0.5. Cold stimulus is extremely positive on the upper and lower limbs. Internal organs
are without pathologies. Make the diagnosis:
Explanation
Vibrating hand tools can cause vibration syndrome, a condition also known as vibration white finger and as Raynaud’s phenomenon of occupational origin. Vibration white finger (VWF), also known as hand-arm vibration syndrome (HAVS) or dead finger, is a secondary form of Raynaud’s syndrome, an industrial injury triggered by continuous use of vibrating hand-held machinery. Vibration syndrome has adverse circulatory and neural effects in the fingers. The signs and symptoms include numbness, pain, and blanching (turning pale and ashen). Of particular concern is evidence of advanced stages of vibration syndrome after exposures as short as one year. Workers tend to underreport the syndrome because symptoms are intermittent and occur most frequently under conditions not present in a doctor’s office (e.g., early in the morning or when the hands are cold or wet).
Early stages of vibration syndrome are characterized by tingling or numbness in the fingers. To be diagnosed as vibration syndrome, these neurologic symptoms must be more persistent and occur without provocation by immediate exposure to vibration. Other symptoms of vibration syndrome include blanching, pain, and flushing. The symptoms usually appear suddenly, and are precipitated by exposure to cold. With continuing exposure to vibration, the signs and symptoms become more severe and the pathology may become irreversible.
From the question stem, the patient is a polisher and uses a grinding machine, these predisposes to vibration disease. Hence, Vibration disease is the best choice here and a preferred choice over Raynaud disease.
170. A woman came to the doctor with complaints of increased body temperature up to 37.8°C and
moderately sore throat for the last 3 days. Objectively: mandibular lymph nodes are enlarged up to
3 cm. Palatine tonsils are hypertrophied and covered with gray coating that spreads to the uvula
and anterior pillars of the fauces. What is the most likely diagnosis?
171. A 57-year-old woman complains of weakness, dyspnea, loss of appetite, and liquid feces. She has
been suffering from this condition for 2 years. Objectively she presents with pale skin, subicteric
sclerae, and bright-red fissured tongue. Lymph nodes are not enlarged. Pulse - 100/min. BP-
105/70 mm Hg. Liver +3 cm, the spleen cannot be palpated. Blood test: erythrocytes - 1.2∙1012/L,
Hb - 56 g/L, color index - 1.4, macrocytes, leukocytes - 2,5∙109/L, eosinophils - 1%, juvenile - 1%,
metamyelocytes - 1%, band neutrophils - 8%, segmented neutrophils - 47%, lymphocytes - 38%,
monocytes - 4%, reticulocytes - 0.1%, platelets - 100∙109/L, ESR - 30 mm/hour, indirect bilirubin -
26 mmol/L. What changes can be expected in the bone marrow puncture material?
172. A 26-year-old woman presents with amenorrhea. 10 months ago she gave birth for a second time.
In her early postpartum period she developed a massive hypotonic hemorrhage. No breasfeeding.
Lately she has been presenting with loss of weight, loss of hair, and indisposition. Gynecological
examination revealed atrophy of the external genitals, the uterus is abnormally small, no uterine
appendages can be detected. What is the most likely diagnosis?
173. A 3-month-old child with signs of rickets presents with positive Chvostek, Trousseau, and Maslov
signs. One day ago the parents witnessed a cyanotic attack in their child - the child broke into a
cold sweat, the eyes bulged, and respiratory arrest occurred. One minute later the child drew in a
loud breath and the child’s condition normalized again. What is the cause of the described signs of
the disease?
174. A 7-year-old boy has severe pulmonary mucoviscidosis (cystic fibrosis). He complains of dyspnea
and blood expectoration. Objectively he presents with lagging physical development, acrocyanosis,
hepatomegaly, drumstick fingers, and nail plates resembling a ”clock face” Provisional diagnosis of
chronic pulmonary heart disease is made. What examination would be the most informative for
diagnosis confirmation?
Explanation
A doppler echocardiography is a diagnostic method for heart related issues. It is a combination of an echocardiogram (which uses sound waves to create an image of the heart) and a doppler technology ( which shows the velocity ie, speed and direction of blood flow in cardiac tissues). An Electrocardiography shows the electrical activity of the heart.
In patients with cystic fibrosis (CF), continuous pulmonary infection and inflammation with thickened secretions cause airways obstruction and hyperinflation. As the disease progresses, these patients develop disabling lung disease and eventually respiratory failure and pulmonary hypertension (PH).
PH is considered to be a consequence of several mechanisms that either raise the pressure downstream of the pulmonary capillaries, induce vasoconstriction, increase blood flow to the lung, or obstruct the pulmonary vessels either by embolism or in situ fibrosis.
The echocardiogram is an integral part of the evaluation of a patient with PH. Common echocardiographic findings in PH includes right atrial and right ventricular (RV) enlargement, reduced RV function, displacement of the intraventricular septum to the left, and tricuspid regurgitation that permits the estimation of the pulmonary artery systolic pressure (PASP).
Therefore, Doppler echocardiography will be the best choice to evaluate a patient with a chronic pulmonary heart disease.
175. A parturient woman is 30 years old, stage I of the labor is ongoing. The fetus is in the cephalic
presentation. Auscultation of the fetal heart sounds detects bradycardia. Evaluation of
cardiotocogram yielded the following data: decrease of basal heart rate down to 90/min., variability
- monotonous (2 and less); late decelerations with amplitude of 50/min. Make the diagnosis and
choose the obstetrical tactics necessary in this case:
176. A 35-year-old man complains of rapidly incresing fatigue, palpitations, “visual snow”, and dizziness.
He has a history of peptic ulcer of the stomach. Objectively the skin is pale. Vesicular respiration is
observed in the lungs. Systolic murmur is detected over the cardiac apex, heart rate is 100/min., BP
is 100/70 mm Hg. The epigastrium is slightly tender on palpation. Blood test: erythrocytes -
3.2∙1012/L, Hb - 100 g/L, color index - 0.95. What type of anemia is the most likely present in this
case?
Explanation[caption id="attachment_1376" align="aligncenter" width="1924"]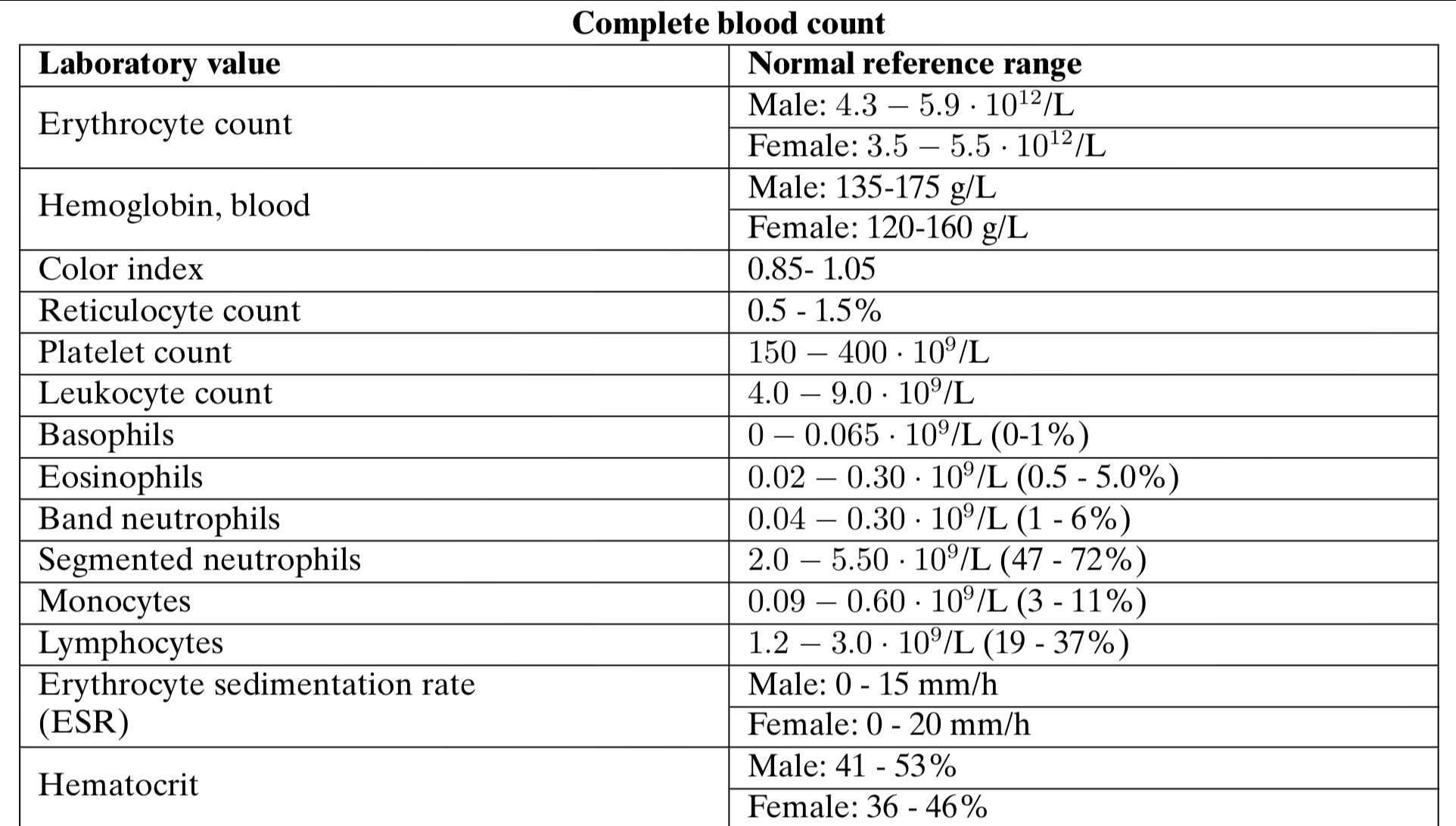 Complete Blood Count[/caption]
Complete Blood Count[/caption]
Anemia is decrease of erythrocytes amount and hemoglobin in unit of blood volume which is accompanied by qualitative changes of erythrocytes.
In men is lower than 4×1012, in women is lower than 3,7×1012 in 1L of blood.
Hemoglobin concentration – in men is lower than 130 g/l, in women is lower than 120 g/l;
Posthemorrhagic anemia is an anemia which develops as a result of hemorrhage. There are two types of anemias of this group according to the character of hemorrhage:
acute posthemorrhagic and;
chronic posthemorrhagic anemia.
Chronic posthemorrhagic anemia develops after repeated hemorrhages, caused by injury of blood vessels during number diseases (ulcer of stomach, hemorrhoids, dysmenorrhea etc.).
Note that that question stem states that he has a history of peptic ulcer of the stomach and one of the complications of peptic ulcer disease is hemorrhage.
Anemias which arise after destruction (hemolysis) of erythrocytes are called hemolytic usually due to mechanical trauma, ionizing radiation, Chemical agents (hemolytic poisons); Biological factors (causative agents of infectious diseases, toxins, enzymes); Immune factors (antibodies).
Iron deficiency anemia arises as a result of: Insufficient iron in organism due to an alimentary anemia in the infants (feeding with cow or goat milk); disorder of iron absorption (resection of stomach, intestines, gastritises, enteritis); increased use of iron in pregnancy, lactation or Hemorrhage which is the most widespread reason of iron deficiency in organism;
However to differentiate posthemorrhagic and iron deficiency anemia:
reduction of color index is typical for iron deficiency anemia, whereas it is often normal in posthemorrhagic anemia.
The patient has a normal color index (0.85-1.05)
177. Mother of a 5-year-old child noticed on the the head of her child a round ”bald” spot 3 cm in
diameter. All the hairs in the focus are broken off at the length of 5-6 mm. The day before the child
was petting a stray cat. Make the diagnosis:
178. For three years a 31-year-old woman has been complaining of pain and swelling of her radiocarpal
and metacarpophalangeal articulations and their reduced mobility in the morning, which persisted
up to 1.5 hours. Two weeks ago she developed pain, swelling, and reddening of her knee joints, her
body temperature increased up to 37.5°C. The treatment was untimely. Examination of the internal
organs revealed no pathologic alterations. Diagnosis of rheumatoid arthritis was made. What
changes are most likely to be visible on the arthrogram?
Explanation
The question stem clearly states that the patient has been diagnosed with Rheumatoid Arthritis.
So basically, we need to differentiate Rheumatoid Arthritis (RA) and Osteoarthritis (OA) so that we can arrive at the correct answer specific for Rheumatoid Arthritis.
RA: autoimmune which erodes articulated cartilage and bone. The inflammatory cells and cytokines then induce pannus (proliferative granulation tissue) formation, deep usurations.
Associated with pain, swelling and morning stiffness, lasting >1hr and the pain improves with use.
Joint findings: joint space narrowing; erosions; juxtaarticular osteopenia; soft tissue swelling; subchondral cysts
Involves Metacarpophalangeal joints; wrist; proximal interphalangeal joints. Does not affect distal interphalangeal joints on the hands
OA: mechanical wear and tear - it’s a degenerative joint disease.
Associated with Pain in weight bearing joints after use (i.e. at the end of the day), and the pain improves with rest.
Joint findings: joint space narrowing; osteophytes (bone spurs); subchondral sclerosis and cysts.
Involves distal interphalangeal joints on the hands (heberden nodes) and Proximal interphalangeal joints (Bouchard nodes); does not affect Metacarpophalangeal joints.
So let’s answer the question:
From the question stem - Radiocarpal (wrist joints); metacarpophalangeal joints were affected with morning stiffness lasting >1.5hrs
These are clearly signs and symptoms of Rheumatoid Arthritis...
From the options it is clear that the only option talking about RA is joint space narrowing; usuration
The other options are talking about Osteoarthritis.
179. A 27-year-old woman, a teacher in the elementary school, complains of frequent stools, up to 3
times per day, with lumpy feces and large amount of mucus, abdominal pain that gradually abates
after a defecation, irritability. Her skin is pale and icteric. Pulse is 74/min., rhythmic, can be
characterized as satisfactory. Blood pressure is 115/70 mm Hg. The abdomen is soft, moderately
tender along the colon on palpation. Fiberoptic colonoscopy detects no changes. What disease can
be suspected?
180. A pregnant woman is 28 years old. Anamnesis: accelerated labor complicated by the II degree
cervical rupture. The following two pregnancies resulted in spontaneous abortions at the terms of
12 and 14 weeks. On mirror examination: the uterine cervix is scarred from previous ruptures at 9
and 3 hours, the cervical canal is gaping. On vaginal examination: the cervix is 2 cm long, the
external orifice is open 1 cm wide, the internal orifice is half-open; the uterus is enlarged to the 12th
week of pregnancy, soft, mobile, painless, the appendages are without changes. What diagnosis
can be made?
181. A 48-year-old woman has arrived to the surgical unit with wounds in her thigh. On examination the
wound surface has dirty-gray coating with unpleasant sweet smell. Wound content resembles
raspberry jelly. Skin tissues around the wound are glossy and turgid. Palpation reveals moderate
crepitation in the tissues. What microflora is the most likely to cause such inflammation?
182. A 65-year-old woman on abdominal palpation presents with a tumor in the umbilical region and
above it; the tumor is 13x8 cm in size, moderately painful, non- mobile, pulsing. On auscultation
systolic murmur can be observed. What is the most likely diagnosis?
Explanation
An abdominal aortic aneurysm is an enlarged area in the lower part of the major vessel that supplies blood to the body (aorta). The aorta runs from your heart through the center of your chest and abdomen.
The aorta is the largest blood vessel in the body, so a ruptured abdominal aortic aneurysm can cause life-threatening bleeding.
Aneurysms can develop anywhere along the aorta, but most aortic aneurysms occur in the part of your aorta that's in your abdomen. A number of factors can play a role in developing an aortic aneurysm, including: Hardening of the arteries (atherosclerosis), High blood pressure, Blood vessel diseases, Infection in the aorta or Trauma.
Most people with abdominal aortic aneurysms don't have symptoms. But symptoms may occur if the aneurysm gets bigger and puts pressure on surrounding organs.
The most common symptom is general belly pain or discomfort, which may come and go or be constant.
Other symptoms may include: Pain in the abdomen or lower back. It may spread to the groin, buttocks, or legs. The pain may be deep, aching, or throbbing, and it may last for hours or days. It is generally not affected by movement.
Another very important symptom is a pulsating feeling over the abdomen.
The tumor mentioned in the question is not referring to an actual tumor literally. It is used to describe the dilated portion of the abdominal aortic aneurysm.
183. The body of a 24-year-old woman with suspected poisoning has been found on the street. Forensic
medical examination was requested by an investigator during examination of the site and the body.
According to the Criminal Procedure Code currently in force in Ukraine, forensic medical
examination is required when it is necessary to determine the:
184. A woman with the pregnancy term of 8 weeks complains of elevated temperature up to 37.6°C, skin
rash that can be characterized as macular exanthema, enlargement of posterior cervical and
occipital lymph nodes, small amount of bloody discharge from the genital tracts. She was examined
by the infectious diseases specialist and diagnosed with rubella. What tactics should the
obstetrician-gynecologist choose?
185. A 59-year-old woman was brought into the rheumatology unit. Extremely severe case of
scleroderma is suspected. Objectively she presents with malnourishment, ”mask-like” face, and
acro-osteolysis. Blood: erythrocytes - 2.2∙109/L, erythrocyte sedimentation rate - 40 mm/hour.
Urine: elevated levels of free oxyproline. Name one of the most likely pathogenetic links in this
case:
Explanation
Scleroderma is a group of rare diseases that involve the hardening and tightening of the skin and connective tissues. Scleroderma affects women more often than men. It results from an overproduction and accumulation of collagen in body tissues. Collagen is a fibrous type of protein that makes up your body's connective tissues, including your skin.
Autoantibodies to basement membrane and interstitial collagens may participate in the pathogenesis of scleroderma. Using the enzyme-linked immunosorbent assay (ELISA), antibodies to interstitial (type I) and basement membrane (type IV) collagens can be detected in the sera of patients with scleroderma (systemic sclerosis).
The primary structure of collagen contains basically 3 amino acids - Glycine, Proline and Lysine. Hence, the elevated levels of oxyproline in this patient’s urine.
Additional Info:
CREST is an acronym for the clinical features that are seen in a patient with this disease. The "C" stands for calcinosis, where calcium deposits form under the skin on the fingers or other areas of the body. The "R", stands for Raynaud's phenomenon, spasm of blood vessels in the fingers or toes in response to cold or stress. The "E" represents esophageal dysmotility, which can cause difficulty in swallowing. The "S" is for sclerodactyly, tightening of the skin causing the fingers to bend. Finally, the letter "T" is for telangiectasia, dilated vessels on the skin of the fingers, face, or inside of the mouth. Usually only 2 of the 5 symptoms of the CREST syndrome is necessary to be diagnosed with the disease.
186. A 57-year-old woman during a regular ultrasound examination presented with a space-occupying
heterogeneous lesion in the right kidney. What is the most informative method of renal tumor
diagnostics?
187. A 25-year-old man was hospitalized with complaints of pain in his lower abdomen and right lumbar
area that appeared one hour ago. Patient’s general state is moderately severe. Body temperature -
38.2°C, heart rate - 102/min. The tongue is dry. The abdomen is painful on deep palpation in the
right iliac area and in the Petit triangle. Aure-Rozanov and Gabay signs are positive. Make the
provisional diagnosis:
188. A 28-year-old woman complaining of irregular menstruations and infertility came to the
gynecological clinic. Menstruations occur since the age of 15, irregular, with delays up to 2 months.
On examination she presents with marked hirsutism and excessive body weight. On vaginal
examination the uterus is reduced in size and painless. The ovaries on the both sides are dense
and enlarged. Ultasound shows microcystic changes in the ovaries, the ovaries are 5x4 cm and
4.5x4 cm in size with dense ovarian capsule. Basal body temperature is monophasic. What is the
most likely diagnosis?
189. The dermatologist has an appointment with a 30-year-old man that complains of severely itching
rashes that especially disturb him at night. The rashes developed 2 weeks ago, after he had
returned from a travel. Objectively on the lateral surfaces of his fingers, hands, wrists, elbows,
lower abdomen, genitals, and thighs there are paired papulovesicles, single pustules, and scratch
marks. What disease can be suspected?
190. An 18-year-old girl was brought into the gynecology deparment with complaints of elevated body
temperature up to 37.8°C, sharp pain in her lower abdomen, more intense on the right, and difficult
defecation. Vaginal examination detected a painful dense elastic formation 5x6 cm in the area of
her right ovary. Pregnancy test is negative. What is the most likely diagnosis?
Explanation
Ovarian torsion, which affects females of all ages, is a gynecological emergency. The main risk in ovarian torsion is an ovarian mass. The most common symptom of ovarian torsion is acute onset of pelvic pain, followed by nausea and vomiting.
Ovarian torsion occurs when an ovarian cyst or mass presents and rotates both the infundibulopelvic ligament and the utero-ovarian ligament. The cyst or mass is usually a benign lesion over 5 cm in diameter.
The ovary, and often the fallopian tube (adnexal torsion), become twisted around their vascular pedicle. The cause of this twisting can be multifactorial. The initial twisting causes obstruction of venous return. This leads to vascular congestion, which causes engorgement and edema. The congestion progresses until arterial flow is compromised, leading to ischemia and infarction. Untreated ovarian torsion can result in complete loss of the ovary, as well as ovarian necrosis and infection.
From the question stem, the pregnancy test is negative, so we can rule out Ectopic pregnancy. A mass of 5x6cm is located around the right ovary, this mass won’t be visible if we have a ruptured cyst.
Ovarian apoplexy (ovarian rupture) – is a sudden rupture (integrity violation) of ovarian tissue, accompanied by bleeding in the abdominal cavity and pain. Similarly, this won’t be the best choice in this case.
191. A 45-year-old man developed constricting retrosternal pain that occurs during walks at the distance
of 200 m. Objectively: heart rate is 80/min., BP is 160/90 mm Hg. During cardiopulmonary exercise
test at 50 W there is a depression of S-T segment by 3 mm below the isoline in V3-V4. What is the
provisional diagnosis?
Explanation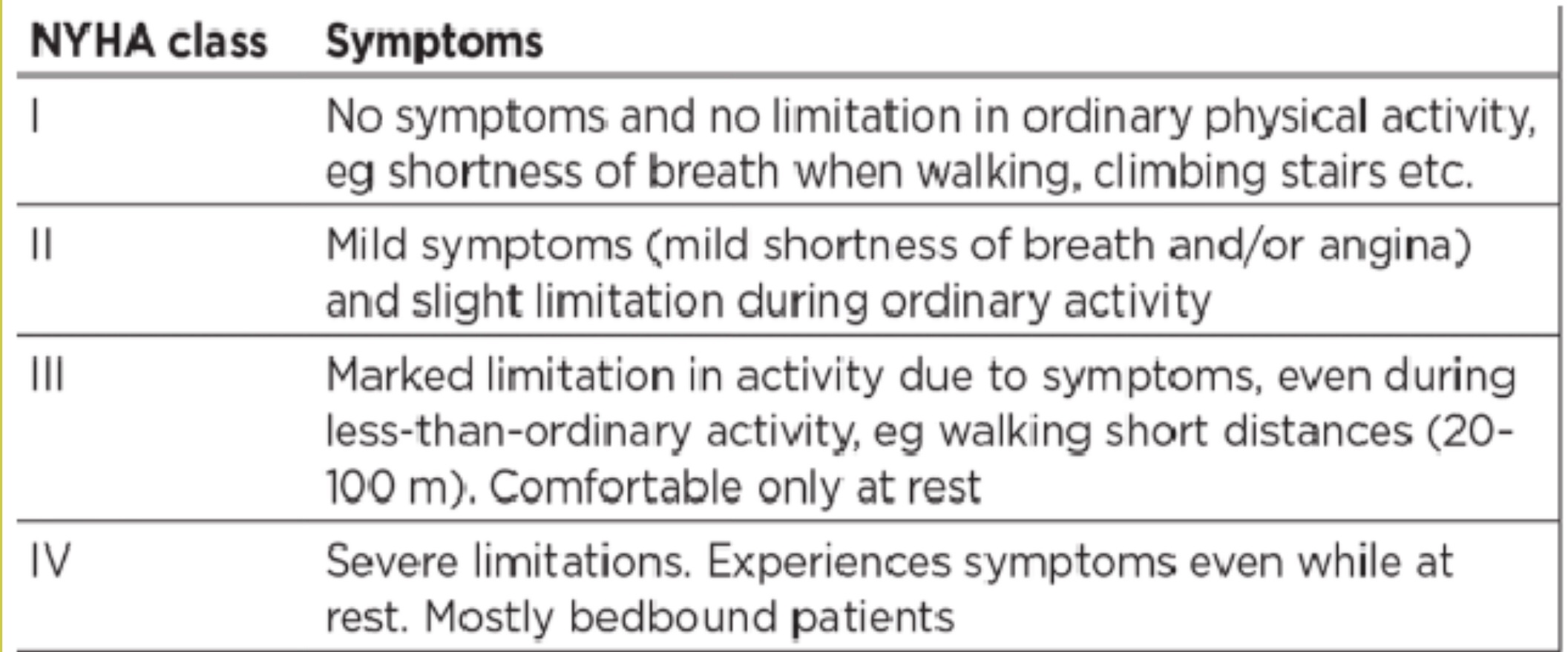
An angina refers to chest pain due to an ischemic myocardium secondary to coronary artery narrowing or spasms. Canadian Cardiovascular Society grading of angina pectoris is a classification used to grade the severity of Angina.
Class 0: Asymptomatic Angina- Mild myocardial ischemia with no symptoms.
Class I: Angina only with strenuous exertion- Presence of angina during strenuous, rapid, or prolonged ordinary activity (walking or climbing the stairs).
Class II:Angina with moderate exertion- Slight limitation of ordinary activities when they are performed rapidly, after meals, in cold, in wind, under emotional stress, during the first few hours after waking up, but also walking uphill, climbing more than one flight of ordinary stairs at a normal pace and in normal conditions.
Class III: Angina with mild exertion- Having difficulties walking one or two blocks or climbing one flight of stairs at normal pace and conditions e.g walking short distances (20 - 100m)
Class IV: Angina at rest- No exertion needed to trigger angina.
The patient in perspective experiences anginal symptoms after he walks about 200m ( a short distance).
The New York Heart Association (NYHA) also classifies the extent of heart failure. It classifies patients in one of the four categories based on their limitations during physical activity.
CLASS I: No symptoms and no limitation in ordinary physical activity
CLASS II: Mild symptoms (mild shortness of breath and/or angina) and slight limitation during ordinary activity.
CLASS III: Marked limitation in activity due to symptoms, even during less than ordinary activity e.g. walking short distances (20 - 100m). Comfortable only at rest.
CLASS IV: Severe limitations. Experiences symptoms even while at rest.
192. A 72-year-old man complains of lower extremity edema, sensation of heaviness in the right
subcostal area, dyspnea at rest. For over 25 years he has been suffering from COPD. Objectively:
orthopnea, jugular venous distention, diffuse cyanosis, acrocyanosis. Barrel chest is observed, on
percussion there is a vesiculotympanitic (bandbox) resonance, sharply weakened vesicular
respiration on both sides, moist crepitant crackles in the lower segments of the lungs. Heart sounds
are weakened, the II heart sound is accentuated over the pulmonary artery. The liver is +3 cm.
What complicated the clinical course of COPD in this patient?
193. To assess the effectiveness of medical technologies and determine the power and direction of their
effect on the public health indicators, the research was conducted to study the immunization rate of
children and measles incidence rate by district. What method of statistical analysis should be
applied in this case?
194. A 5-year-old child was brought to the ENT department by an ambulance. The child presents with
cough and difficult respiration. From the patient’s history it is known that the child was playing with a
toy construction set, when suddenly started coughing and developed labored breathing.
Examination detects periodical cough, labored expiration, and respiratory lag in the left side of the
child’s thorax. Auscultation: diminished respiration on the left. Percussion: tympanitis. X-ray shows
a displacement of the mediastinal organs to the right. Make the diagnosis:
Explanation
The question says it all already.
The child was playing with a toy and presented with labored breathing and cough. On examination, there is a respiratory lag on the left. On auscultation, there is diminished respiration on the left and on X-ray, there is a mediastinal shift to the right. This clearly shows the foreign body (toy) was lodged in the left bronchus.
If the foreign body were to be in the trachea, there will be no respiration in both lung fields. It won’t be localized to only one side.
To differentiate if it is a complete or valvular bronchostenosis. Take a close look at the X-ray report - displacement of the mediastinal organs to the right. (Mediastinum is the space and organs located between both lungs i.e. the heart, aorta, thymus, trachea etc).
In complete bronchostenosis, air cannot enter or leave the left bronchus so the volume of the left lung will remain the same while in valvular bronchostenosis, air can enter the left lungs but cannot come out. Therefore, in valvular bronchostenosis, there is a gradual increase in the left lung volume which eventually shifts the mediastinum towards the right side.
195. In April during the medical examination of various population groups, 27% of individuals presented
with low working ability and rapid fatigability. The following symptoms were observed in the affected
individuals: swollen friable gingiva that bleeds when pressed, hyperkeratosis follicularis not
accompanied by skin dryness. These symptoms most likely result from the following pathology:
196. A 45-year-old woman is registered for regular check-ups due to Werlhof disease (immune
thrombocytopenia). Complete blood count: Hb - 100 g/L, erythrocytes - 2.8∙1012/L, platelets -
90.0∙109/L, leukocytes - 8.4∙109/L, erythrocyte sedimentation rate - 13 mm/hour. Examination
detects a single small hematoma on the anterior surface of the thigh, developed after the patient
accidentally stumbled on a table. What treatment tactics should be chosen in this case?
197. A 23-year-old man has accidentally swallowed brake fluid. After that he has been presenting with
anuria for 5 days already; his creatinine levels elevated up to 0.569 mmol/L. What treatment tactics
should be chosen in this case?
Explanation
Indications for Dialysis:
Plasma Urea >30mmol/L
Creatinine >600mcmol/L
Hyperkalemia>6mmol/L
Metabolic acidosis (HCO3 <10mmol/L)
Uraemic encephalopathy
Fluid overload and pulmonary edema
Uraemic pericarditis
GFR < 15mls/min
Oliguria (less than 200ml in 12 hours)
Anuria (0-50ml in 12 hours)
Patient had Anuria for 5 days plus elevated creatinine - Dialysis
Types of Dialysis:
-
Hemodialysis: countercurrent flow of blood and dialysate (usually acetate or bicarbonate
-
Hemofiltration: Removal of plasma and its dissolved constituents
-
Peritoneal dialysis: uses peritoneum as a semipermeable membrane
The typical reference range for serum creatinine is 60 to 110 micromoles per liter (μmol/L) (0.7 to 1.2 milligrams per deciliter (mg/dL)) for men and 45 to 90 μmol/L (0.5 to 1.0 mg/dL) for women.
Reference ranges for Laboratory values are usually given at the end of your question paper. Check the last few pages during exams to confirm the reference range used. We also have the Lab values on this site.
198. A 20-year old man, a calibrator of dosimetry equipment, committed a gross violation of safety regulations, when he put two ampoules with cobalt-60, each with the radioactivity of 7 MCi, in the pockets of his trousers and jacket. He has been keeping the ampoules in his pockets for 8 hours. The tissues at the distance of 0.5cm from the source received the dose of 30Gy (3000R), while the tissues at the distance of 20cm - 2R. Did this man develop radiation sickness?
199. Indicators of work of inpatient departments in the city hospitals for the past year were analyzed. After that the meeting was held at the central city hospital and, based on the results of the analysis, a decision was made to decrease the number of beds in the inpatient departments, and instead open daycare units with partial hospitalization in the city polyclinics. What is the main goal of this decision?
200. A 65-year-old man complains of dyspnea, severe cough with expectoration of small amounts of blood-streaked sputum, weight loss, body temperature 37.2*C, loss of appetite, and weakness. He has been suffering from this condition for years. The patient’s condition deteriorated one year ago, dyspnea developed 3 weeks ago. The patient is a lifelong smoker. He is a carpenter by occupation. Objectively he is of normal body type but emaciated. Right side of the chest is retracted, excurcions are limited, accessory muscles take part in the respiration, respiratory rate is 22/min. Percussion detects dull sound over the right upper segment. Chest X-ray shows shrunken right upper lobe with homogeneous shadow connected to the root of the lung; the root is deformed; mediastinal organs are displaced to the right. What is the most likely diagnosis?
Explanation
Atelectasis is a partial or complete collapse of the entire lung or a specific area, or lobe, of the lung, leading to impaired exchange of carbon dioxide and oxygen. From the question, the Chest X-ray confirms this: shows a shrunken right upper lobe. Also, the right part of the chest is retracted and percussion sounds are dull (if the lungs were to be filled with air, resonance sounds would be heard).
Further radiographic findings such as, changes in the mediastinum and diaphragm, facilitate diagnosis. As the lung volume decreases with atelectasis, the mediastinum shifts towards the affected field on the radiograph. Furthermore, a unilateral elevated diaphragm increases the suspicion for atelectasis.
Pneumothorax will produce resonance sounds on percussion, not dull sounds as seen in this patient. Tuberculosis and Sarcoidosis can present with hilar lymphadenopathy and a well circumscribed granuloma on chest X-ray (Tuberculosis - caseating granuloma; Sarcoidosis - non caseating granuloma).